Chapter VII. Uterus And Female Genital Tract. Uterus-Cervix And Endometrium
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Chapter VII. Uterus And Female Genital Tract. Uterus-Cervix And Endometrium
Malignant disease of the uterus is comprised almost exclusively of two lesions: epidermoid cancer of the cervix and adenocarcinoma of the endometrium. The more common is the cervical disease, but both are important and the clinical manifestations, as well as the screening and diagnostic measures, overlap greatly. The two will be considered in sequence.
Cancer of the uterus is of major importance for the following reasons:
1. Carcinoma of the cervix and endometrium account for a combined incidence of 40,000 and mortality of 14,000 women yearly in the United States.
2. Absolute prevention of a sizable percentage of the cervical lesions is possible today. It has been estimated that up to 80% of cervical cancer would not occur if routine circumcision of newborn male infants was practiced.
3. Death from cancer of the cervix is almost 100% preventable. Widespread application of a simple, inexpensive, accurate screening procedure (cytology) would detect the early, completely curable cervical lesion.
4. The control measures to be described are well within the average physician's time, experience, and equipment.
Cervix. Epidemiology. Incidence
29,000 new cases per year 11.5% of female cancer incidence
Mortality
10,000 deaths per year
8.1% of female cancer mortality
Rates
Incidence per 100,000 women | 31.5 |
Mortality per 100,000 women | 10.8 |
Age
Significant increase beyond age | 25 |
Over 75% of cases occur between ages | 35-70 |
Trend Last Ten Years
Incidence-increase of | 9% |
Mortality-decrease of | 41% |
A distinction must be made between carcinoma in situ and invasive cancer (see below). The average age at diagnosis of carcinoma in situ is less than 40 years; of invasive cancer, about 46 years. The significance of this will be dealt with below. The incidence of cancer of the cervix diminishes after the age of 65 years.
Other Factors
1. Women with cancer of the cervix commonly have one or more of the following characteristics:
(a) Married
(b) Often several marriages or multiple sexual partners
(c) Many children
(d) Low socioeconomic status
(e) Negro
(f) Non-Jewish
2. Epidemiologic studies have shown that these characteristics stem from the two basic factors important in the etiology of cancer of the cervix.
(a) Age at beginning of regular coitus. Women with cervical cancer are quite likely to have married at an early age. The malignant lesions in these instances may be due to the sensitivity of young cervical tissue to carcinogenic stimuli or may be related to the degree of sexual activity of younger couples.
(b) Circumcision status of the marital partner. Cervical cancer is quite rare among women whose husbands were circumcised in infancy. Conversely, cervical cancer occurs predominantly among women whose husbands were not circumcized. This is presumably due to a poor state of penile hygiene and accumulation of smegma under the foreskin in uncircumcised males.
3. The status of chronic cervicitis, lacerations, and other benign lesions as precursors of cancer is not clear. Some believe that they are important predisposing factors and that good obstetric and gynecologic care affords a measure of cancer prevention.

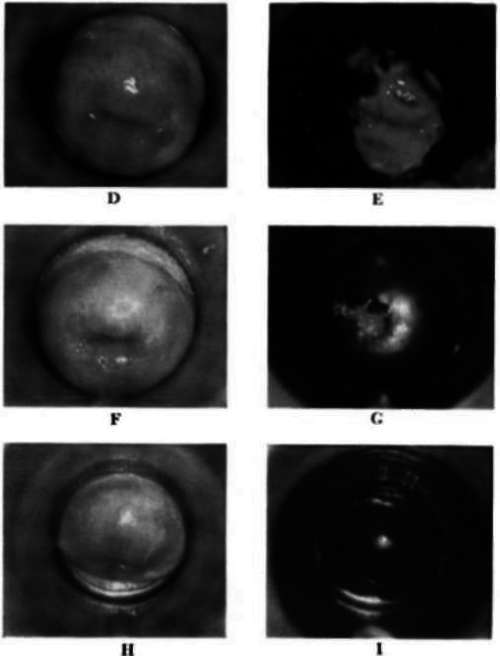
Plate 2
A, Leukoplakia of the cervix before iodine. B, Leukoplakia of the cervix after iodine. C, Cervical polyp without iodine. D, Chronic cervictis before iodine. E, Chronic cervicitis after iodine. F. Carcinoma in situ of the cervix before iodine. G, Carcinoma in situ of the cervix after iodine. H, Normal-appearing cervix before iodine. I, Normal-appearing: cerxix after iodine. Papanicolaou cytologic examination revealed carcinoma in situ of the cervix.
4. It is often stated that women with carcinoma of the cervix are likely to have had a large number of pregnancies. This is frequently the case, but the fact that such women have married at an early age appears to be more important than the number of children per se in predisposing them to cervical cancer.
5. The role of other factors, such as douching, the use of contraceptives, induced abortions, etc., is thus far undetermined.
Trends
A decrease in the mortality of cancer of the cervix has been noted in some areas in recent years. This decrease is probably due to earlier diagnosis and treatment of lesions and better obstetric and gynecologic care. Total hysterectomy is a more commonly employed operation now, and this precludes development of carcinoma of the cervical stump.
Etiology
The factors of early age of first marriage and regular coitus plus lack of circumcision of the male partner are, as mentioned previously, significant predisposing conditions.
Recently, studies have suggested that women with a history of major therapeutic x-ray exposure to the pelvic region have an increased risk of cervical cancer. The risk is greater for carcinoma of the endometrium and vulva, but apparently the cervix is not exempt from hazard. The validity of such observations has been denied by some, however.
Premalignant lesions
Leukoplakia is regarded by some as a precancerous condition of the uterine cervix.
There is increasing agreement that the major cytologic atypias, as well as certain dysplasias or dyskeratoses, should be assigned to the category of premalignant lesions.
Continue to:
My Books

