Distribution Of Polyps Of The Rectum And Colon
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Distribution Of Polyps Of The Rectum And Colon
On the basis of figures compiled on autopsy and surgical specimens, most workers believe that polyps and cancer have a closely parallel distribution throughout the rectum and colon. The distal bowel is the most common site, about 75% of all polyps and cancer arising in the rectum or rectosigmoid areas (Fig. 68). The remaining 25% are distributed more or less evenly from the cecum to rectosigmoid.

Fig. 68. Distribution of adenocarcinomas of the rectum and colon detected as a result of routine sigmoidoscopy in a presumably well population.
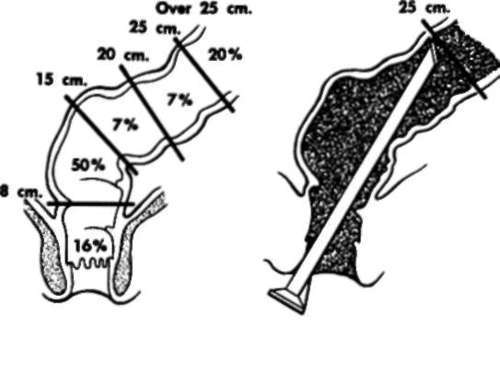
Fig. 69.

Fig. 70.
20% of all polyps are boyond the reach of the sigmoidoscope.
16% only of all polyps are within the reach of the examining finger.
64%, or roughly 2/3, of all lesions occur above the reach of the examining finger but within the reach of the sigmoidoscope.
Fig. 69. Distribution of polyps of the rectum and colon detected as a result of routine sigmoidoscopy.
Fig. 70. Relative value of sigmoidoscope and examining finger in the detection of lesions of the rectum and lower colon.
Figures reflecting experience with routine sigmoidoscopy are somewhat different. About 80% of polyps detected clinically are located in the rectum or rectosigmoid (Fig. 69). The fact that the remaining large area of proximal bowel accounts for only 20% of the polyps is a reflection of the difficulties encountered in the x-ray detection of polyps of the colon, as well as the fact that x-ray studies of the colon are seldom performed routinely.
Several important lessons are to be learned from Figs. 68 and 69, including:
1. The great importance of sigmoidoscopy in the detection and diagnosis of these lesions. Approximately three fourths of all polyps and cancer of the rectum and colon are within reach of the 25 cm. sigmoidoscope (Fig. 70).
2. The relative ineffectiveness of digital rectal examination in the detection and diagnosis of polyps and early cancer. This is in direct contradiction to most textbook maxims, which base their conclusions on series including a large proportion of bulky, often prolapsing, advanced tumors, easily felt with the index finger. In a detection program screening essentially asymptomatic adults, only 13% of carcinomas of the rectum and colon were within reach of the examining finger (Fig. 71). In other words, seven out of eight cancers would have been missed if reliance had been placed on digital examination alone to the exclusion of sigmoidoscopy.
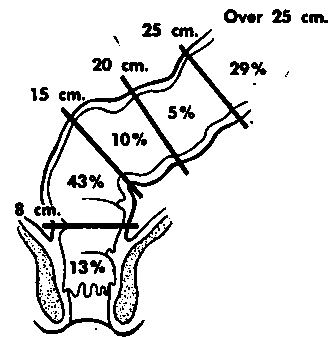
Fig. 71. Distribution of carcinomas of the rectum and colon detected sigmoidoscopically.
Incidence Of Polyps In Presumably Well Adults
As previously mentioned, the incidence of simple polyps increases progressively with advancing years, and males are affected more commonly than females in a ratio of 3 to 2 or 2 to 1 (see Fig. 66).
Relationship Between Polyps And Cancer
No discussion of the pathology of cancer of the rectum and colon would be complete without consideration of the relationship of benign adenomas (polyps) to carcinomas in this area.
Before attempting to reach a conclusion on the subject, let us consider the evidence pro and con in the following brief, sometimes oversimplified form.
Are benign polyps the precursors of cancer of the rectum and colon?
Yes
1. The areas of distribution of polyps and cancer in the rectum and colon are almost identical.
2. Polyps are found much more frequently in bowels that are the site of cancer than in normal mucosa.
3. Polyps found in association with an obvious cancer are more likely to be malignant than polyps occurring by themselves.
4. Atypical or frankly malignant changes are a fairly frequent finding in clinically "benign" polyps.
5. The gross and microscopic appearance of many obvious cancers is such as to strongly imply origin in a polyp.
6. In a few instances it has been possible to watch a frank cancer develop in or at the site of a polyp undisturbed over a period of years.
7. The incidence of cancer in a polyp 's directly related to its size; i.e., the larger the polyp, the more likely it is malignant.
8. In familial polyposis (an admittedly extreme example) the progression from benign polyp to cancer is obvious, observable, and almost 100%.
No
1. The supposed similarity of distribution of polyps and cancer is misleading and more apparent than real.
2. Polyps do not undergo malignant degeneration. They arc malignant from the onset or not at all.
3. Microscopic cancer in a polyp is not, and most often will never become, clinical cancer.
4. Polyps are extremely common lesions. Most people with them never develop cancer.
5. Many lesions are erroneously called polyps but are not true adenomas.
6. Cancer can arise de novo without any pre-existing or associated polyps.
Majority opinion would appear to favor the affirmative viewpoint. The principles that logically follow then are as follows:
1. Most, but not all, cancers of the rectum and colon arise from pre-existing benign polyps.
2. Areas of mucosal hyperplasia may be the precursors of polyps.
3. The length of time it takes a cancer to undergo the sequence from hyperplasia to polyp to carcinoma is unknown. This latent period is most likely measured in years.
4. Not all, perhaps not even the majority of, polyps become cancer. There is, however, no way of predicting which harbor this malignant potential and which will remain benign. Empirically, therefore, they must all be regarded as potentially malignant and treated as such.
5. Detection and removal of polyps of the rectum and colon afford a unique opportunity for cancer prevention.
Ulcerative Colitis And Cancer
The relationship between carcinoma of the rectum and colon and ulcerating colitis may be summarized as follows:
1. Over-all incidence of subsequent cancer development is 3 to 10%.
2. The risk is increased, often to several times the preceding figures, by the following:
(a) Long duration of disease (especially over ten years)
(b) Widespread involvement of the bowel with ulcerative colitis
(c) Presence of pseudopolyps (especially multiple)-not because they themselves are premalignant lesions, but because their presence usually denotes a markedly abnormal, cancer-prone mucosa (see below)
3. When cancer does become superimposed on ulcerative colitis, the outlook is often poor because:
(a) The cancer tends to be multicentric in origin, affecting several areas of the bowel simultaneously.
(b) The lesions tend to be quite undifferentiated in type.
(c) The diagnosis is often delayed and difficult because of the already altered state of the bowel.
(d) The patient's general condition after years of chronic illness may compromise diagnosis and management.
4. The pseudopolyps seen in ulcerative colitis bear no relationship to the other polyps described except that of gross appearance. Cancer that does occur does not appear to arise in the polyps per se but rather in the chronically inflamed and damaged adjacent mucosa.
Continue to:
My Books

