Pathology. Classification Of Carcinoma Of The Rectum And Colon
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Pathology. Classification Of Carcinoma Of The Rectum And Colon
The vast majority of all the malignant tumors occurring in the colon and rectum are adenocarcinomas of varying degrees of differentiation. Squamous carcinoma of the anal canal is a relatively rare lesion but is important because of its accessibility.
For purely descriptive purposes, classification is most logically made according to gross appearance. From the viewpoint of prognosis, the classification is based on microscopic features.
Classification according to gross appearance
The classification according to gross appearance is shown in Fig. 64.
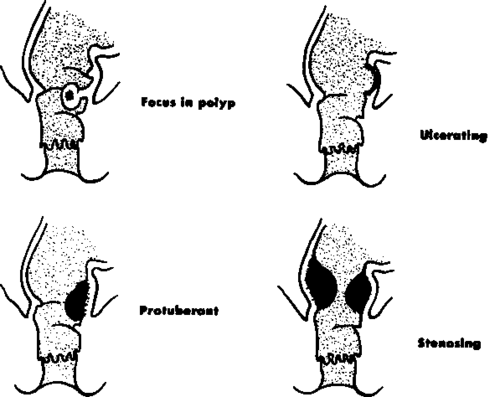
Fig. 64. Cross classification of malignant lesions of the rectum.
Classification Based On Microscopic Features
Dukes. Carcinoma of the rectum and colon ordinarily grows more by penetration than by lateral or longitudinal extension along the wall.
The Dukes classification divides lesions into three stages according to the degree of penetration of the bowel wall and the presence or absence of lymph node metastasis (Fig. 65).
In general, the lower the stage, the more favorable the prognosis and vice versa.
Many modifications of this classification have been proposed since its introduction in 1932. For the most part they represent a refinement of the principles set down here.
Broders. This classification acknowledges the fact that, in general, the more undifferentiated a lesion is, the greater its tendency to invade and metastasize and, therefore, the poorer its prognosis.
This rule has many apparent exceptions, but when this classification is combined with the Dukes method, a fairly reliable and practical basis is laid for estimating prognosis.
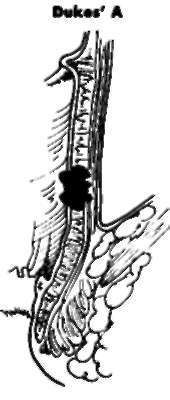
Confined to rectal wall.

Outside rectal wall; no lymph node metastases.

Regional lymph node metastases.
Fig. 65. Dukes' classification of carcinoma of the rectum and colon.
Under the Broders system the tumor is examined microscopically and an estimate made of the relative proportion of differentiated and undifferentiated adenocarcinoma cells. The resultant figure expressed in a percentage allows one to assign it to one of four grades:
Grade | % of differentiated cells |
1 | 75-100 |
2 | 50-75 |
3 | 25-50 |
4 | 0-25 |
Many other systems of microscopic classification have been proposed, but those of Dukes and Broders have stood the test of time and are the most widely used.
Incidence Of Cancer In Presumably Well Adults
The incidence of cancer of the rectum and colon in presumably well adults subjected to sigmoidoscopy shows the same progressive increase with age (Fig. 66) as does that of simple polyps, their supposed precursors.
It is true that most of the lesions that formed the basis for the graph shown in Fig. 66 were not of the conventional variety-i.e., large, bulky, often ulcerating and bleeding, sometimes obstructing and certainly symptomatic neoplasms, frequently palpable by means of the index finger. More often they were small sessile or pedunculated polypoid lesions, detectable only by the sigmoidoscope, without evidence of obstruction, ulceration, or bleeding, and usually asymptomatic. It is probably just as true that the principal difference between these two types of lesions is one of time-i.e., one represents a later stage of the other.
This fact should serve to emphasize once more the importance of routine periodic sigmoidoscopy.
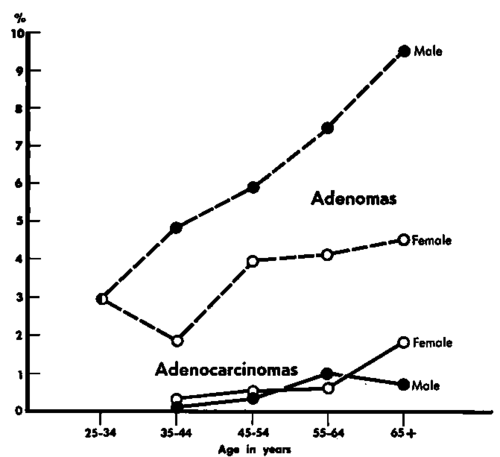
Fig. 66. Incidence of adenocarcinomas and adenomas (polyps) of the rectum and colon detected by routine sigmoidoscopy in a presumably well population. The vertical column on the left represents the percentage of persons examined with positive findings.
Continue to:
My Books

