Steps In The Diagnosis And Initial Management Of The Thyroid Cancer Suspect
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Steps In The Diagnosis And Initial Management Of The Thyroid Cancer Suspect
1. Look for thyroid cancer whenever a patient presents with nodes in the neck and the primary lesion is not obvious.
2. Careful palpation of the thyroid gland and neck with special reference to:
(a) Character of the gland, e.g., multinodular or uninodular.
(b) Character of the suspicious lesion:
(1) Discrete or diffuse?
(2) Hard or soft?
(3) Regular or irregular?
(c) Evidence of infiltration and fixation of adjacent structures.
(d) Presence of cervical adenopathy.
3. Indirect laryngoscopy to look for presence of recurrent laryngeal nerve involvement with vocal cord palsy.
4. X-ray studies of the following:
(a) Chest and neck, being careful to include the thoracic inlet for possible substernal extension or pulmonary metastases. The presence of tracheal compression, calcification within the gland, and other findings should also be noted.
(b) Bones for possible distant metastases if clinically indicated.
5. Rule out the presence of toxicity by clinical assessment and appropriate laboratory studies, e.g., protein-bound iodine, basal metabolism test, radioiodine uptake studies, depending on the preference of the physician and the facilities available.
6. Consider the possibility of thyroiditis. As a result of the inflammatory and necrotic process, in the classical case of thyroiditis there will be evidence of an acute onset, with considerable local pain, warmth, and swelling plus a markedly elevated blood protein-bound iodine and sharply diminished uptake of I131 by the gland.
7. Scintigram. After a dose of radioactive iodine, the gland can be scanned with a monitor and a "map" or scintigram made. The nodule can be evaluated from the standpoint of its affinity for the isotope. In general, the findings are interpreted as follows:
(a) When the lesion concentrates the radioactive iodine, it is referred to as a "hot" nodule and is thought more likely to be benign (Fig. 41).
(b) When the lesion picks up little or no iodine, it is termed a "cold" nodule and is thought more likely to be malignant (Fig. 42). Such information taken in conjunction with all the other clinical findings may help in determining which nodules should be removed.
8. Advise surgery, the type of operation to be determined by findings at the time. Aspiration biopsy is not recommended because of the limitations of accuracy. The specific indications for recommending surgery for thyroid lesions deserve further elaboration.
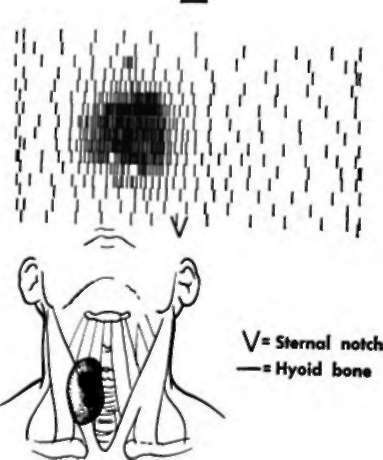
Fig. 41. "Hot" nodule, right lobe of thyroid gland. (Courtesy Dr. Richard Benua.).
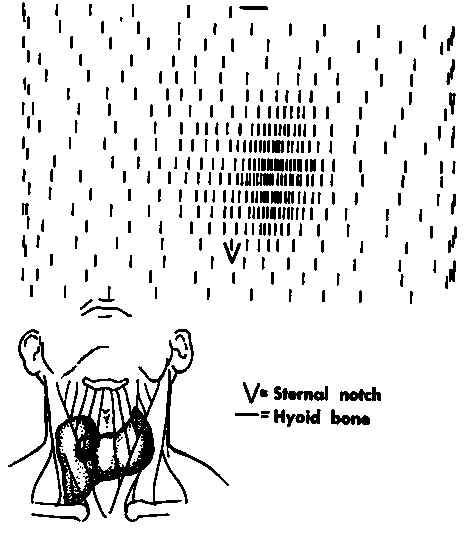
Fig. 42. "Cold" nodule, right lobe of thyroid gland. (Courtesy Dr. Richard Benua.).
Continue to:
My Books

