Renal-Cardiovascular Diseases. Pathological Effects Of Steroids. Continued
Description
This section is from the book "The Scientific Contributions Of The Ben May Laboratory For Cancer Research", by The University of Chicago. Also available from Amazon: The Scientific Contributions Of The Ben May Laboratory For Cancer Research.
Renal-Cardiovascular Diseases. Pathological Effects Of Steroids. Continued
Salt-Loading
During most of this century some clinical investigators have considered that a higher than necessary dietary intake of sodium chloride plays some role in the cardiovascular diseases in man. The reduction in blood pressure achieved by restriction of salt intake and, more recently the demonstration, of the anti-hypertensive effects of natriuretic agents lend support to this view (Smirk et al., 1960). We have confirmed the observation of Meneely et al., (1953) that high dietary loads of sodium chloride cause severe hypertension and renal-cardiovascular damage in unilaterally nephrectomized rats and somewhat milder changes in intact rats (Fig. 4). The development of these changes in the salt-loaded rat is greatly affected by adrenalectomy, as we have shown (Crane & Ingle, 1959) , but the correlation between availability of adrenal hormones and pathological changes is not complete. Even in the adrenal insufficient rat there is still a positive correlation between salt-load, elevation of blood pressure, and pathological changes in the heart and kidney, and current experiments (to be published) show that if the unilaterally nephrectomized, adrenalectomized rat is salt-loaded for 6 months and longer, it can develop hypertensive vascular disease in the absence of any replacement therapy with adrenal hormones. Adrenal cortical insufficiency delays but does not permanently prevent the damaging effects of long-term salt loading. It seems improbable that saltloading causes an increase in the secretion of adrenal steroids; all the available evidence indicates that a high salt load causes a significant suppression of the secretion of aldosterone, the most potent sodium-retaining compound known among the natural steroids. But since salt-loading does not wholly abolish the secretion of adrenals steroids, the basal secretion by the adrenal cortices may have some obligatory sodium-retaining action. The adrenalectomized rats drink less water than do the non-adrenalec-tomized rats when both groups receive the same load of sodium chloride but no exogenous hormone (Crane & Ingle, 1959). It may be supposed that the adrenal-insufficient animal can rid itself of sodium chloride more easily than can the eucortical animal and that, for this reason, the pathological effects of a salt load are diminished, but we have not fully tested this hypothesis.
The salt-loaded, adrenalectomized rat with one kidney removed is very sensitive to the administration of adrenal cortical extract (ACE) (Crane et at., 1959). Doses of ACE which are too small to correct all the metabolic aberrations of adrenal cortical insufficiency cause hypertension in animals given a diet containing 4 per cent salt. Here again we assume that the intact adrenal glands can suppress the secretion of sodium-retaining steroids to a significant extent, but the rat given a uniform intake of ACE, although small, may still have a fixed excess of exogenous sodium-retaining hormone co-existing with a deficiency of glucocorticoids. It is possible to cause nephrosclerosis and cardiovascular damage by giving doses of ACE much smaller than those required to maintain optimal resistance of adrenalectomized rats to severe stress (Ingle & Nezamis, 1949).

Fig. 4. Kidney from a rat given sodium chloride diet by stomach tube for 84 days. There are glomerular lesions, protein tubular casts and hypertensive arteriolar thickening. Blood pressure 170 mm. Hg. H. & E.X210.
Adrenal Regeneration
It was discovered by Skelton (1959) that hypertension, associated with pathological changes, develops if one adrenal gland is removed and the other gland is enucleated and allowed to regenerate in unilaterally nephrectomized rats given 1 per cent saline to drink. This experimental observation has been confirmed by us (Crane, 1960) and by other investigators (Masson, Koritz & Peron, 1958). Hypertensive pathological changes begin to appear in the arteries of the heart, kidney, and other viscera around the fourth week of adrenal cortical regeneration and are well established at 8 weeks (Fig. 5). The animals bearing regenerating cortical tissue drink more saline than the normotensive control rats; this difference is especially marked at the time when hypertensive pathological changes first develop. Hypertension can be prevented by the substitution of tap water for saline as drinking fluid and also by carefully transplanting the regenerating cortical tissue into the spleen or liver.
Regeneration of cortical tissue proceeds from the subcapsular layer of glomerulosa cells which remains after enucleation, and these proliferate to show an eightfold increase in cortical cells throughout the experimental period. Since aldosterone is produced by the subcapsular glomerulosa layer of the adrenal, it has been postulated that 'adrenal regeneration hypertension' is caused by a relative or absolute hyperaldosteronism. This has not been confirmed by analyses of adrenal vein blood from rats with regenerating adrenal cortices (Brogi & Pellegrino, 1959), nor in experiments conducted in vitro (Masson, Koritz & Peron, 1958). An alternative hypothesis has been suggested, namely, that the hypertensive syndrome is related to a period of temporary adrenal cortical insufficiency, after which there is an increased reactivity of the arteriolar bed to a normal steroid pattern and electrolyte level as the animal returns to the eucortical state (Page et al., 1958). Groll-man (1958) subscribed to a similar view but holds that the hypertension is probably related to potassium depletion associated with the initial period of adrenal cortical insufficiency. In our experiments, the return to eucor-ticalism, as measured by the restoration of thymic weight to normal, is associated with the maximum increase in saline consumption and the development of hypertension and hypertensive pathological lesions. It may well be that the elevation of blood pressure is connected in some way with electrolyte imbalance, either potassium depletion or sodium excess, but the exact role which the regenerating adrenal cortical tissue and its secretions play in this altered homeostasis remains obscure.
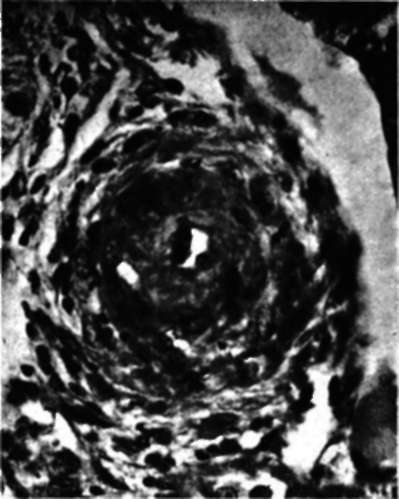
Fig. 5. Kidney from a rat bearing regenerating adrenal cortical tissue, maintained on 1 per cent sodium chloride for 40 days. A small renal artery shows hypertensive proliferative sclerosis and intimal thickening Blood pressure 182 mm. Hg. H. & E. x.
Atherogenic diets. We have reported on the experimental induction of obesity, hyperlip-aemia, and hypercholesterolaemia by feeding rats with a high fat diet rich in egg yolk which under certain conditions leads to severe atherosclerosis, coronary occlusion, and myocardial infarcts (Wilgram, 1959). Atheromatous lesions occur in both the presence and absence of the adrenal glands and neither unilateral nephrectomy nor salt-loading is necessary for their production. The atherosclerotic lesions produced by dietary methods are localized principally to the vascular intima in contrast to the medial type of lesion observed in the hypertensive salt-loaded rats.
Ischaemia and other forms of renal injury. Laboratory procedures of various kinds which injure the kidney in a variety of ways are followed in the rat by a predominantly hypertensive type of vascular disease. Procedures causing renal damage that have been used include hypervitaminosis, sulphonamide injections, the administration of antikidney serum, choline deficiency, partial nephrectomy, and mechanical interference with the supply of arterial blood to the kidney (Wilgram & Ingle, 1959). When the renal lesion is extensive, hypertension can develop in the absence of salt-loading. Although these procedures lead to several different patterns of renal injury, a hypertensive type of vessel change seems to be the common response.
Aging
Animals develop degenerative diseases as they age even when they are kept under environmental conditions that could hardly cause them any stress. Some of the changes that occur in female breeder rats discarded at about 1 year of age from the Sprague-Dawley farms have been described (Ingle & Baker, 1953; Ingle, 1956). Some rats develop hypertension, a few have ulcers of the stomach, while renal and cardiovascular lesions can be found in almost every animal. Although the aetiology of the vascular damage is undoubtedly complex, we suspect that obstructive lesions in the renal tubules may play an important role. A calcifying type of arteriosclerosis rather than atherosclerosis occurs frequently and a form of polyarteritis is occasionally seen. As these animals approach 2 years of age, every one of them develops a tumour of some form, mostly mammary fibroadenoma, but sometimes carcinoma. These animals have been raised in air-conditioned rooms, the entire colony is free from infectious diseases, and diet is optimal for growth, reproduction, and lactation. Repeated breedings are the only possible source of stress; these female rats have each cast 6 litters of young at 7-week intervals before being discarded at about 1 year of age.
Continue to:
My Books

