Fractures Of The Neck Of The Femur. Part 2
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
Fractures Of The Neck Of The Femur. Part 2
If there is no impaction, splintage with extension is required. Treatment by mobilisation and massage may still be carried out with benefit, provided that the extension is applied on any system other than that of the Hodgen type. The method of administering a dose of relaxed movement to the knee of a patient who has been put up in a Thomas' knee-splint is shown in Fig. 83. It is possible, when the splint is slung from an overhead support, to perform the manipulations single-handed, but the difficulties are considerable and the strain is great. The assistant raises the end of the splint; the masseur then, loosens the sling which supports the limb just below the level of the knee-joint. He now grasps the limb firmly below the knee-joint, and receives the weight of the limb on to his forearm as each successive sling towards the ankle is released. It is essential that the next sling above the knee should be in close proximity to it and should adequately support the lower part of the thigh. The assistant then loosens the extension. The masseur, skilled in the treatment of recent injury and in the administration of relaxed movement, is now able to give a dose of mobilisation while still exerting powerful extension on the lower fragment of the broken femur via the knee-joint. On completion of the relaxed movement the assistant refixes the extension before the masseur adjusts the slings. For accuracy extension and slings may be marked, if this precaution seems desirable. It is sometimes urged that this treatment cannot fail to impede union and to allow movement of the fragments and the return of deformity. The limited movement will assist in formation of callus, and, as regards the second assertion, the only effect on the fragments is that the masseur, by his grip, transforms the tension on the fragments into that employed when a Hodgen splint is used. Far from disturbing the position of the fragments, his manipulations render possible a painless reduction of deformity. By these means it is often possible to secure a muscular relaxation which assists restoration of outline of the bone more readily than any other means short of open operation. Photographs of two patients who sustained gunshot wounds of femur, and who were treated on the lines indicated, are shown in Figs. 84 to 87.
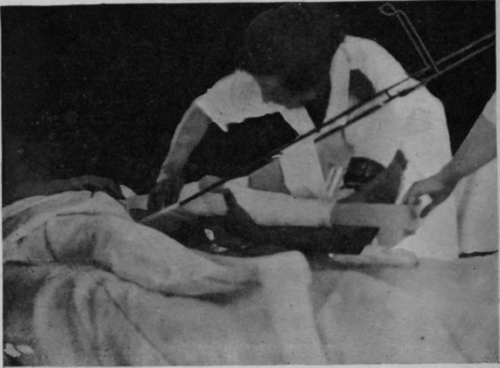
Fig. 83. - To show the administration of a dose of relaxed movement to the knee-joint of a patient with fractured femur, before union is firm enough to allow removal of the extension. It was in this manner that treatment was given to the patient shown in Figs. 86 and 87 on and after the tenth day from the receipt of a septic "G.S.W." of middle third of the shaft of the femur. The ordinary surgical treatment of the wound, drainage, irrigation, subsequent sequestrotomy, etc., was carried out concurrently.
The surgeon who lacks the requisite assistance or the temerity to undertake this treatment in person need not withhold all physical treatment. Much may be done without mobilisation of the knee in the early stages. Thus an attempt, with considerable hope of success, can be made to keep the muscles from becoming adherent to the bone at the site of fracture by means of graduated faradic contraction. The patella can be cept comparatively mobile, and stroking of the whole limb and movement of toes and foot-joints should be performed during the early stages. The ankle may be moved if the appliance permits. No other massage movement need be given till union is complete. In septic compound fractures union is often delayed, callus formation is sluggish, circulation very faulty, and oedema equally intense. Great benefit can be bestowed in these cases by kneading. Every movement will tend to shake the fragments, and it is necessary, therefore, that great care and gentleness should be exercised, and that any pressure exerted, however slight, should find something to counteract it on the other side of the limb. If necessary this must be one of the masseur's hands. Granted these requisites, the movement of the fragments will stimulate the callus and hasten recovery; excess will delay and even prevent union. The question of restoring function and regulation of splintage is considered in Chapter XXXII (The Combination Of Massage And Splintage In Orthopaedic Surgery).
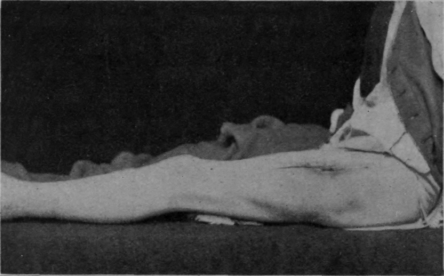
Fig. 84. - This and the subsequent photo were taken of a patient before discharge from the Special Surgical Hospital, Shepherd's Bush. He sustained the ordinary septic "G.S.W." of femur on August 24th, 1918. He was treated on a Thomas' knee splint. Massage and relaxed movements were begun on September 21st. Flexion through 55° was secured by the middle of October. A month later he was taken off individual treatment and placed in a special class for exercise without weight, and by the 25th November his knee could be bent to a right angle. The muscular development and power is shown in Fig. 85.
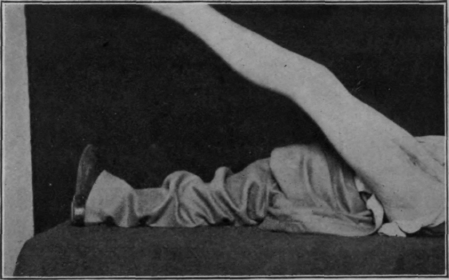
Fig. 85. - Same patient as that shown in Fig. 84. Note the power of full extension of the knee and general "good condition." Photo taken (about) March 3rd, 1919. There was no visible deformity or shortening.
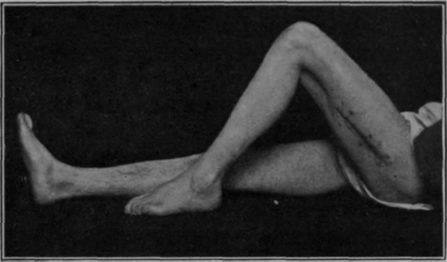
Fig. 86. - The second of seven cases who were taken off individual massage treatment, and treated thenceforth in a "special class" for exercise within three months of sustaining septic gunshot wounds of the femur.
History: -
"G.S.W." .... September 2nd, 1918.
Massage and movements . September 12th, 1918.
Started use of sliding seat . October 30th, 1918.
special class . . . November 26th, 1918.
Sequestrotomy . . . January 29th, 1919.
Photo (about) . . . March 3rd, 1919.
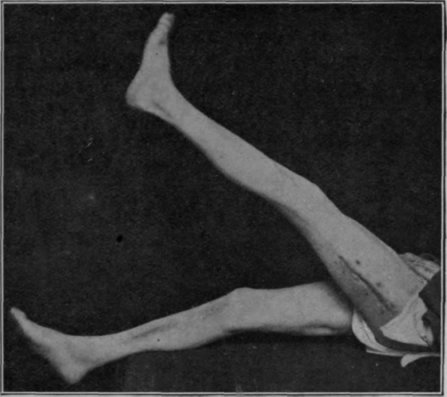
Fig. 87. - The same patient as that shown in Fig. 86. The photos were taken about six months after receipt of wound. Treatment began in both cases shown while the "through and through" wounds were widely open. The cases were kindly sent to me for treatment by Mr. Trethowan.
Continue to:
My Books

