Fractures Of The Neck Of The Femur. Part 3
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
Fractures Of The Neck Of The Femur. Part 3
The same remarks apply to all fractures of the femur below the neck. Any movement is prescribed by the surgeon, though it were well if, in recent fractures, he would always try the effect of mobilisation under the influence of massage before deciding on open operation for the reduction of deformity. When union is complete and the patient is handed over to the masseur for restoration of function, the first attempts at movement should always be performed so as to ensure that no strain falls upon the site of fracture. At first any strain exerted should be in the line of the long axis of the limb, lateral strain being added by very slow stages. A Thomas' knee-splint is the most suitable splint on which the limb can be put up, if we wish to apply massage to any case of fracture of the shaft of the femur.
As already indicated, treatment by mobilisation is considerably hampered by any form of splintage which requires the body-weight as an extension. Under these circumstances the knee must be kept immobile until such a time as union is complete. Much has been written about, and the strongest advocacy has been given to, the use of calliper extension, the traction usually acting from the condyles of the femur. My experience of the after-results of these cases is that full extension is seldom secured while the calliper is in place (see Fig. 88), and a knee that lacks the last 10° of full extension is a poor thing at best. Far more useful is full extension, even at the expense of a loss of the possibilities in flexion.
The best restoration in outline of the shape of a broken femur is usually secured by open operation, but the cases that show such excellent alignment after operation are just those which tend to present insuperable difficulties in adjustment when other means are tried. On the other hand, when operation is rendered difficult owing to comminution, treatment by mobilisation yields its most satisfactory results in restoring the contour of the bone.

Fig. 88. - To show the application of a common form of calliper extension as applied to a fractured femur. Note that full extension of the knee is impossible, as the top of the shin meets the cross of the calliper before this position is reached.
In sum, then, if it is possible to reduce the deformity without operation, treatment by mobilisation and massage offers the best chance of exact restoration; it hastens the formation of callus and, therefore, the restoration of weight-bearing functions; and it maintains more nearly intact the mobility of the joints, the muscular power and co-ordination, than any other method of treatment. But, even if full treatment is withheld, at least let us be sure of this: better it is to have a short leg and a sound foot than a perfect leg and a painful foot. In other words, in all cases of fractured femur let us remember that we are treating a patient and not merely a bone, and that it is our duty, as far as in us lies, to let no portion of our patient suffer from neglect. The toes, foot, ankle and patella should never be overlooked. It is often well to remember that the patient has two legs!
The remarks made on the inhibitory action of synovial fluid on callus formation, after fractures of the humerus into the elbow-joint, apply with equal force to those involving the kneejoint. Early mobilisation is advantageous, and only requires the most careful graduation.
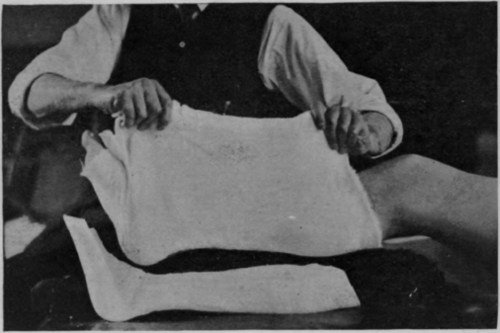
Fig. 89 - To show how a leg may be raised from a posterior gutter splint by means of a "cradle" of lint before union is consolidated.
After any fracture of the leg, massage of the thigh can be used to restore the vaso-motor tone by reflex, and to assist the circulation by its mechanical effect and by toning up the muscles of the arterioles. Hence great benefit can be bestowed, although the leg itself may be fixed in plaster. If massage is ordered after fracture of the fibula above its lower third, the treatment may proceed without fear of displacement. Surface stroking of the whole limb is followed by general massage of the thigh, and movement is given to all joints, with the exception of eversion of the foot. Movement must be carefully supervised by the surgeon till union, which often takes place rapidly, is complete.
The same remarks apply to fracture of the tibia alone, but movements must be much more guarded, varying from comparative freedom, corresponding to that usually applicable to fracture of the fibula, to the almost negative amount that it is possible to apply if both bones are broken. The best guide is to be found in the amount of tearing of the natural internal splint - the periosteum - and this can only be estimated by the mobility of the fragments, which in turn is indicated by the amount of displacement after accident. If there was little displacement, the graduation may be rapid; if great, mobilisation must be reduced accordingly.
If the shafts of both bones are broken, great care must be exercised in the earlier stages. Until union is complete the splint must be either incomplete or one that is easily removable without disturbing the fracture. If there is small chance of the fragments moving out of place, it usually suffices to place the limb in a posterior gutter plaster of Paris splint (see Fig. 89). The limb rests on a sheet of lint which is not attached to the splint. By means of this the limb can be lifted from the splint without any fear of disturbing the fragments. It is then rested on a suitable support and treatment is given, care being taken to see that the original position of the foot is maintained throughout treatment. Hence the importance of the grip of the left hand as shown in Figs. 5, 6, and 7, pp. 28 - 30. Stroking of the whole limb may be given first, then the limb is replaced in the splint and gentle kneading of the thigh follows. The treatment terminates with movement of the toes. When union is complete - it is more rapid towards the upper end of the tibia than towards the lower - knee and hip movements may be commenced gradually, though great care must be taken to avoid any transverse strain being placed on the site of fracture. The limb is then placed at rest and the ankle is mobilised separately. At the earliest opportunity the patient is allowed to swing the leg over the side of the bed, and re-education in walking is commenced (see Chapter XX (Re-Education In Walking).). This should be about five days after union is complete, i.e., probably during the third week.
Continue to:
My Books

