Massage And Splintage In Orthopaedic Surgery. Part 2
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
Massage And Splintage In Orthopaedic Surgery. Part 2
Then let us consider for a moment the final stages of treatment. The scientific manner in which the use of a walking calliper should be terminated is a matter of close co-operation. To maintain its use for a given number of days, weeks, or months, and then to discard it altogether on a stated day means one of two things: either its use has been maintained too long, or great risk attends the discarding. During the whole of the period which elapses between the day when union is sufficiently firm to allow relaxation of the extension, to some six or eight weeks prior to the day when we anticipate that the calliper may be discarded, the patient should be encouraged to perform muscle training first, and then exercises without weight. During the last few weeks that the calliper is to be worn, one, or, better still, two portions of the day should be set aside during which the patient is taught co-ordination exercises which entail a gradually increasing use of the weight-bearing function of the limb. This can most conveniently be accomplished by use of the sliding-seat, the stationary bicycle, and by re-education in walking as described in a previous chapter (see Chapter XX (Re-Education In Walking).). The first fortnight should see the patient advance up to the point where he "rocks to and fro" while maintaining his grip on the back of a chair. By the end of the second fortnight he should be able to take a few regular steps, or even walk across the room unaided, and the third fortnight should see a daily advance in the distance travelled and in rapidity of movement, particularly at all turning points of his progression. If all goes well we can then be reasonably certain that the patient is ready to leave off his calliper while moving on the flat by himself, and this he is allowed to do.
He is next allowed to begin ladder work for all four limbs under supervision, as a preliminary to stair-work under supervision and, finally, alone, and meanwhile the diurnal period of activity without the calliper is increased. By this time the patient may be considered to be safe for short periods morning and evening, walking about without a calliper, provided the ground is dry and reasonably even. He should not be allowed out in wet or slippery weather, or on rough ground, without his calliper until he is able to advance with his training up to the full use of a skipping-rope.
The advantages of this method of treatment may be summarised thus: -
(1) The re-education in functional use is gradual. (2) Errors in co-ordination are corrected at the outset and the formation of bad habits, leading of course to limping, are avoided.
(3) The gradual return of function ensures that, if union is not sufficiently firm to allow freedom in use, the defect may be recognised at the earliest possible moment.
(4) The discarding of the calliper is thus rendered safe, or, if not, (the converse of 3).
(5) We have a ready method of putting our opinion as to the nature of the union to the test, and of recognising that we are in error as to its solidarity before any serious damage has been done.
(6) With this sure test at our disposal it is safe to make tentative experiments in weight-bearing, at an earlier stage than is possible if we ignore the graduated restoration of function.
(7) Individual treatment is not essential; five or six patients can be dealt with quite easily by one masseur at the same time in class.
But in all these things it is manifest that the closest cooperation is essential between all three principals: the patient, the masseur and the surgeon. And so it is throughout the whole realm of orthopaedics.
If the masseur is effectively to co-operate with the surgeon, it is essential that both should fully appreciate the principles which underlie the application of splintage. Splints are applied to afford support to a broken bone, to limit movement at a joint, and to rest some structure or to stretch another, or possibly to effect both ends at the same time.
Whenever a patient is ordered massage, it is incumbent on the surgeon to explain the raison d'etre of any form of apparatus worn. Whatever its use, however, the discarding thereof should always be controlled by principles similar to those laid down for the discarding of the walking calliper.
Thus, whenever external splintage is used to support a bone after fracture, the nature of the splints employed can be altered, the area splinted can be reduced, and the time during which the splints are worn may be altered from day to day. Take, for example, a simple fracture through the shaft of the radius and ulna in their middle thirds. The splintage first applied is shown in Fig. 79 (p. 156), and consists of a long posterior splint from hand to axilla and a shorter anterior splint. Four to seven days after fracture the anterior splint can be discarded. Almost invariably by the end of the second week the long posterior splint can be replaced by a posterior metal splint which reaches from olecranon to metacarpo-phalangeal joints. The elbow is bent to a right angle, and the bandage around the splint is attached to the patient's neck or to the sling so as to ensure that full supination is constantly maintained. A very short anterior splint may be worn for a few days if deemed advisable (see Fig. 158). Up to this point the patient has spent most of his days recumbent with the distal end of the splint resting on a pillow, the palm of the hand facing upwards. Now he is allowed up, sitting or walking all day, and the former position is resumed at night only. The end of the third week sees the patient free from his supinating appliance, and two days later the metal splint is replaced by one made of corrugated cardboard. This is shortened daily and made narrower on alternate days, till, by the end of the week, it is only a narrow slip, two inches broad, and the wrist is left free. About this point it may be necessary to sling the patient in pronation one day and in supination the next.
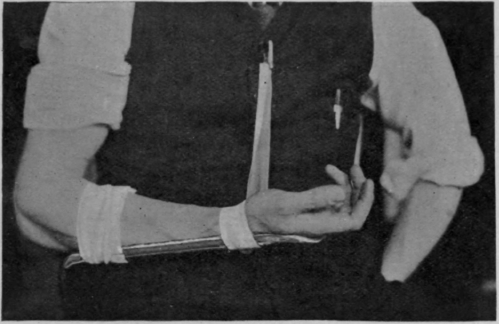
Fig. 158. - To show how a forearm may be slung in supination while a short metal splint is still worn.
Continue to:
My Books

