Massage And Splintage In Orthopaedic Surgery. Part 5
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
Massage And Splintage In Orthopaedic Surgery. Part 5
Whenever a splint is used to rest a weakened muscle the principles which underlie its application must be respected during treatment. Thus, if a patient is wearing an abduction splint to rest a weakened deltoid, free abduction from the horizontal upwards to the vertical and full rotation may be administered, either by the masseur or by the aid of apparatus, e.g., the overhead weight and pulley. If the splint supports the arm more or less in the horizontal plane, then the limb should not be lowered below this level while the patient is sitting or standing. When he is recumbent, however, the weight of the limb is no longer liable to be supported by the deltoid, and so, theoretically, a greater degree of movement may be allowed in this position. In practice, however, the necessity rarely arises and, should it do so, care should be taken to see that during adduction the head of the humerus is not drawn downwards in the glenoid, but is rather pushed well home in an upward direction.
So, too, when treating a patient who wears a cock-up splint, there is little or no chance of overstretching any of the long extensor muscles, provided the hand is kept in full supination when unsupported. When in pronation, however, every care must be taken not to lower the hand beyond the straight line. This is not intended to imply that a few extra degrees of flexion would injure the extensors, even were they completely paralysed. The point really is this: For the purposes of treatment - massage, loosening, re-education - no movement beyond the straight line is essential, and there is certainly a point not very far removed from this position where injury to the muscles would ensue if the hand were allowed to rest there for any considerable length of time. Further on, in palmar-flexion, there is doubtless a point to which even momentary movement would inflict injury. We have nothing to guide us as to where either of these points may be, so it is imperative to take no risks. The limit fixed must therefore be arbitrary, and that suggested above allows a greater freedom than many physico-therapists will grant. One more detail, often overlooked, and yet of ever-increasing importance as greater freedom in treatment becomes permissible: full flexion at the metacarpo-phalangeal joints (and probably at the more distal joints as well), should be administered in full dorsi-flexion of the wrist only; no flexion should be allowed at these joints when the wrist has been lowered to a straight line.
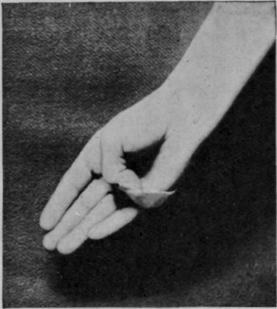
Fig. 162. - To show how the opponens pollicis can be prevented from stretching by the application of adhesive plaster. If desired the nail need not be covered, as the plaster can be split and made to encircle the distal phalanx.
The punctilious care with which adequate support is provided for a dropped wrist, a dropped ankle, or a paralysed deltoid is altogether laudable. No less, however, do other paralysed muscles need similar treatment if their recovery is to be expedited or even allowed to take place. Beyond all question the most important individual muscle in the upper extremity is the opponens pollicis, and yet in respect of treatment by rest it is probably the most neglected. All that is required is a loop of adhesive strapping placed round the thumb, the other end passing over the ulnar border of the hand (see Fig. 162). So, too, in cases of paralysis of the posterior tibial nerve it is rare to find precautions taken to rest either the transverse adductor or the lumbricals. Yet, should these fail to recover, metatarsalgia is inevitable. If applied early enough, a strip of adhesive plaster placed around the foot behind the heads of the metatarsals (after these have been well moulded into position), is often adequate. Hyper-extension at the metatarso-phalangeal joints is well-nigh impossible while the anterior metatarsal arch is fully maintained - though why this should be I do not know.
Probably the form of splint for a paralysed muscle which most closely approximates to the ideal is the toe-elevating spring for external popliteal paralysis, especially if the spring is arranged so as to exert an inverting influence on the foot. It allows, but limits, the freedom of action in the antagonists; it saves weakened muscles from overstretching while, at the same time, allowing them freedom for activity when power is returning. But even so it is not perfect, as the spring will not replace the tibialis anticus in so far as it is concerned with the support of the longitudinal arch of the foot. So we have to beware lest this tends to give way, and, if it does, we have to be content with a far from ideal device, namely, a valgus T-strap attached round the outside iron.
When we consider the possibilities of applying a similar device to a hand after section of the ulnar nerve, it is easy to understand why splintage for this condition is so often unsatisfactory, and why we are so often faced with the necessity of restoring the resulting deformity. In the first place, a loop of strapping passing over the dorsum of the proximal phalanx and fixed to the palm should serve to prevent the last 45° of extension of the metacarpo-phalangeal joints. Then a light splint should be attached to the dorsum of the proximal phalanx, and from this a jury-mast should project in a straight line, carrying from its extremity a loop which should prevent flexion of the two distal joints beyond about 30°. Even this arrangement ignores the paralytic condition of many other muscles, and would entail the manufacture of such a flimsy affair, that, in practice, the ideal is unattainable. The only makeshift possible is to employ either an anterior or a posterior splint with one bend in it opposite the metacarpo-phalangeal joints, which will keep these joints bent to about 6o°. The two distal joints will then remain approximately straight (see Fig. 164).
Continue to:
My Books

