Re-Education In Walking. Part 4
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
Re-Education In Walking. Part 4
All the ordinary leg and foot exercises may now be undertaken, but a word is necessary as to their performance.
The patient stands with the weight of the body on the outer borders of his feet; the inner borders need not be completely raised, but should bear little weight. The heels and toes are kept parallel and the feet about four inches apart. The knees are kept rigidly in full extension. The body-weight is then thrown on to the heels and is gradually transferred forwards till most of the weight is on the head of the fifth metatarsal (see Fig. 118). A close watch must be kept at this point to avoid a most deleterious action. It is essential that the plantar concavity of the anterior metatarsal arch should be maintained. Otherwise the weight is liable to be taken on the heads of the fourth and fifth metatarsals, and this will lead to a "splaying" of the foot in this position - one of the causes, when permanent, of the pain of metatarsalgia. A kind of circling movement is now performed which throws the weight more and more towards the inner side of the transverse metatarsal arch, the heels meanwhile being raised slightly (see Fig. 119). The toes are then turned inwards and the heels out, and the exercise is repeated. The third stage is to reverse the position (heels together, toes out) and repeat. If there is any tendency to flat-foot, this exercise should be omitted until muscular strength is sufficiently restored to ensure that there shall be no strain on the plantar ligaments. The same applies to the exercise illustrated in Fig. 114, p. 275.
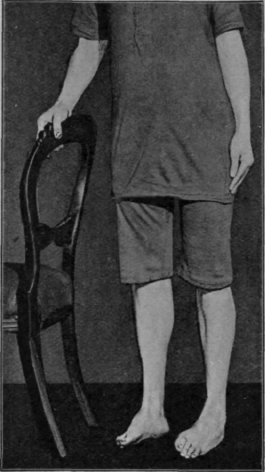
Fig. 120. - To show the raising of the inner side of the feet while the toes perform the "clawing" exercise.
Raising and lowering the inner sides of the feet, which are placed parallel to one another again (see Fig. 120), "clawing" meanwhile, forms the fourth part of the exercise, while the fifth consists of standing on the heels and raising the toes (see Fig. 121). The sixth and last is the ordinary heel-raising-knee-bending exercise, but this should be performed in at least two positions, one with the feet parallel and the knees touching (see Fig. 122), the other with the toes apart and heels together (see Fig. 123). No matter how far the toes may be everted, care should be taken to ensure that the limb bends so as to maintain the long axis of the thigh parallel with that of the foot. Another point to remember is that patients are usually allowed to perform this movement far too rapidly. The heels should be raised to their full extent and the knees driven firmly backwards before any bending is commenced. The bending should be performed very slowly and very gradually, and the patient should "squat" on the heels while he counts "three" very slowly before returning to the original position on tip-toe with the knees taut.
These six (or seven) several exercises should be regarded as various parts of a single exercise. In the massage-room they should be performed once, a few minutes' massage follows, and then they are performed again. As soon as the patient can be relied upon to perform the exercise efficiently, he is instructed to do so twice or three times a day. Thus on getting out of bed in the morning he does it once, a second time after shaving, a third after his bath, and so on up to eight or ten times. The "spacing" of the exercise is most important.

Fig. 121. - To illustrate the exercise in which the patient stands on the heels. Note that the inner borders of the feet are raised more than the outer.
Skipping is invaluable as a finale in treatment, while tip-toe walking, "goose-step," and heel walking all have their place.
Bicycling on a stationary bicycle can frequently be started at an early date. Not only may the pedals be driven round and round, but they may also be rocked to and fro with advantage.
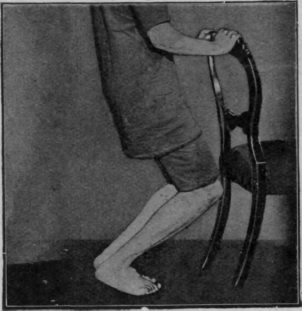
Fig. 122. - The first heel-raising-knee-bending exercise. Note the knees fall directly over the toes. The feet are kept parallel.
The aim is not so much to regain strength as to re-educate coordination. If we wish materially to build up the strength of our muscles by the use of a bicycle, we go for a ten to fifteen mile ride. Few patients would be able to spend two hours or more on a stationary bicycle. The monotony alone is too fatiguing. By tightening the resistance it is supposed to be possible to do a great amount of work in a short time. Few of us, I think, would be foolish enough to elect to ride in the teeth of a contrary wind or to tackle an adverse hill in the early stages of training in the open. It is common knowledge that these things act detrimentally owing to fatigue. Why then attempt them in the course of re-education?
"Kneeling-trunk-falling" is often of great service (see Fig. 124). As pointed out in a previous chapter (see p. 182), it is essential to regard and strengthen the lower fibres of the vastus internus in nearly all cases of leg injury.
Before the patient is discharged, an attempt must be made to impress the necessity of walking with heels and toes parallel, of standing with the toes slightly turned in while the knees are kept well braced back, and of avoiding the "toes-out-knee-bend" position, Which is so easily acquired and so hard to discontinue. It is often wise to build up the heel of the boot or shoe on the inner side by one third to half an inch. This ensures the maintenance of the correct position of the feet, but the patient must be impressed with the vital importance of conscientiously performing the true "heel-and-toe" movement, and of stiffening the knee from the moment the heel touches the floor until it leaves it again. If more attention were devoted to training the quadriceps when treating cases of flat feet, this distressing condition would be found to be far more amenable to treatment.
Continue to:
My Books

