Re-Education In Walking. Part 5
Description
This section is from the book "Massage Its Principles And Practice", by James B. Mennell. Also available from Amazon: Massage It's Principles and Practice.
Re-Education In Walking. Part 5
Thus is performed the re-education in walking. Once allow a patient to limp for any length of time, and he may acquire a life-long habit, which may, in turn, lead to grave disability out of all proportion to the original injury.
Modifications are required to suit each individual case, but the general principles should always be observed.
In this as in all remedial exercises the most important point to observe, if success is to be ensured, is so to arrange the exercises that progress may be made day by day, and that each addition is so slight that the patient's muscles are unable to recognise any increase in the strain put upon them.
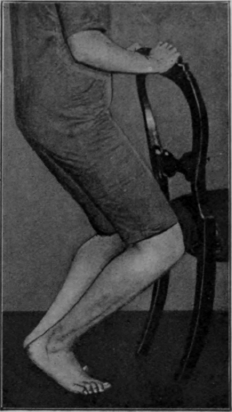
Fig. 123. - The second heel-raising-knee-bending exercise. Note the knees still fall directly over the toes. The feet are at about an angle of 90° to one another.
It will be noticed, in the description of the re-education, that every care is taken to ensure against any dropping of the longitudinal arch of the foot; but, if this has taken place and the patient is flat-footed, all the joints in the foot must be loosened thoroughly by manipulation, and then the re-education exercises will provide a perfect scheme for the restoration of the disability, though those described for the treatment of metatarsalgia may be added with advantage. (See Chapter XXXI (The Treatment Of Deformities).) If actual deformity is present, exercises can sometimes relieve the patient to a certain extent; but to secure perfect restoration it is often necessary to place the limb in plaster after a thorough wrenching of all the joints of the foot. As a preliminary, if the case is acute, and the foot swollen, blue, and cold, general massage to benefit the circulation should be given for a few days while the patient is kept in bed. In addition, free "bed gymnastics" should be prescribed if the patient is to receive full benefit from treatment. All the muscles should be exercised regularly, but without placing the foot on the floor. When the plaster has been removed the patient must be warned forthwith that under no circumstances is he to stand on the floor without wearing shoes with heels raised on the inner side, as already described, or to allow his weight to fall on the inner side of his foot during the exercises. It is well to remind the patient that even when taking a bath he must stand in such a position that the longitudinal arch is maintained. His trouble has been due to the stretching of the structures in the sole. The moulding of the foot has relaxed them, but has not shortened them again; it has only made shortening possible. This takes time, and, if they are stretched again once only, the good acquired by weeks of patient work can be undone in five minutes.
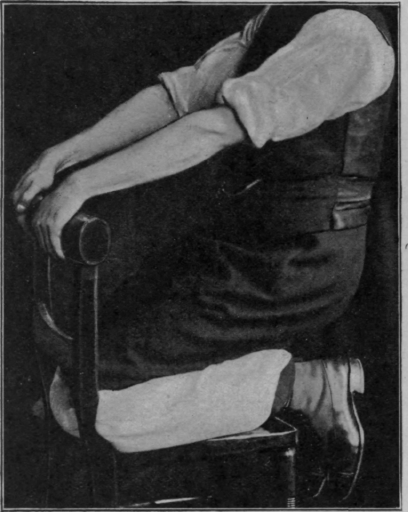
Fig. 124. - The end position of kneeling-trunk-falling and raising.
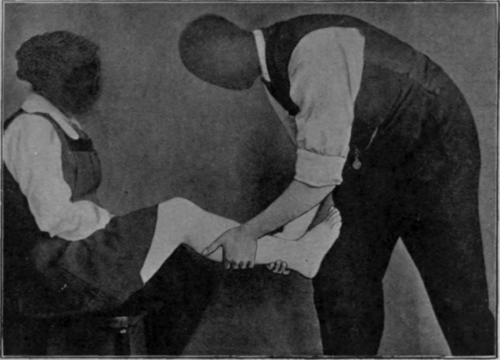
Fig. 125. - To show one method of attempting to stretch the tendo Achillis.
The "clawing" with feet crossed is also designed to arrest the dropping of the anterior metatarsal arch and subsequent metatarsalgia. Should this develop it is important to secure relief at once by strapping the arch, pending the restoration of the foot by the exercises. Assistance can also be afforded by inserting pads behind the heads of the metatarsals or by placing a bar of leather, half an inch deep - as on a football boot - under the sole. This bar is commonly placed much too far forward. The first metatarsal head usually rests in a shoe at a point just in front of the place where the sole is made first to touch the ground. The bar, therefore, as a rule, should be so arranged that the weight is borne on a part of the sole which, in ordinary life, does not touch the ground at all. It should be unnecessary to add that the bar should be applied obliquely across the sole, as the outer end must rest entirely behind the head of the fifth metatarsal. At first it is a matter for surprise how far back in a boot this point really lies.
This device is often of service in the treatment of claw-foot. The disability commonly arises from insufficiency of the tendo Achillis. The bar, by dorsi-flexing the foot in walking, naturally entails the stretching of the tendon, and every exercise should be devised to assist the process. Massage for this condition sometimes helps to an appreciable extent. The patient should sit facing the masseur, who stands with one foot forward and knee bent. The patient places his foot flat on the inclined plane formed by the masseur's thigh (see Fig. 125). The inclination is gradually reduced while deep lateral manipulation of the calf is performed. The tendon itself may be vibrated. All the extensors of the toes require stretching, and here again the vibrator is very useful. It is essential that all the joints in the foot should be loosened as thoroughly as possible, especially the tarso-metatarsal joints.
The treatment of foot deformities and of metatarsalgia will be considered later (see Chapter XXXI (The Treatment Of Deformities).).
Continue to:
My Books

