Cardiac Hypertrophy
Description
This section is from the book "A Manual Of Pathology", by Guthrie McConnell. Also available from Amazon: A Manual Of Pathology.
Cardiac Hypertrophy
In this condition there is an increase in both the number and size of the muscle fibers. It may be the result of either outside interference to the heart's action, as in adhesive pericarditis, particularly if pericardium is also adherent to surrounding tissues; or inside resistance, as occasioned by valvular lesions. It also occurs when there is increased resistance to the flow of blood, as is found in arteriosclerosis.
Hypertrophy will, however, occur only when the heart is primarily able to overcome the obstacle. If unable to do so, there will be relaxation, dilatation. As a rule, one chamber of the heart is chiefly involved, but it is unusual not to find other chambers more or less affected.
When the heart enlarges sufficiently to overcome its obstructions and the circulation is carried on without any apparent trouble, the condition is known as compensatory hypertrophy. This may continue for a long time, but there finally comes a moment when the heart is no longer able to do its work. The symptoms then of failure of compensation make their appearance.
According to the location of the obstacle different cavities of the heart are involved. In the most common valvular lesion, mitral regurgitation, there is a hypertrophy of the left ventricle. In lesions of the aortic valve the greatest enlargement may occur, giving rise to the "cor bovinum." Enlargement of the left ventricle may follow stenosis of the aorta, from an increased resistance to the flow of blood through the peripheral arteries as in various forms of arteriosclerosis or obliterating endarteritis, and from certain forms of nephritis.
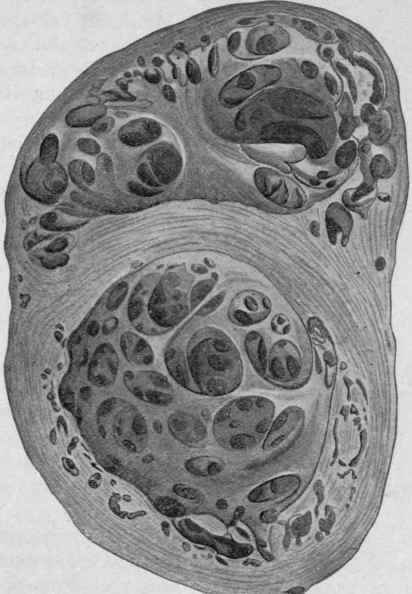
Fig. 134. - Hypertrophy and Dilatation of the Heart (Bollinger).
Enlargement of the right ventricle arises from interference with the circulation within the lung, as in emphysema, chronic bronchitis, and asthma.
The hypertrophy resulting from valvular lesions is due to the cavity containing a greater amount of blood than is normal, whether stenosis or insufficiency or both be present. If there is stenosis, the entire charge of blood is not pushed forward before the heart enters into diastole and receives another supply from the auricle. If there is regurgitation the ventricle during its diastole receives blood both from the auricular and from the distal sides. In either case the heart must increase its muscular power before the circulation can be properly carried on.
Continue to:
My Books

