Nephritis, Inflammation Of The Kidney
Description
This section is from the book "A Manual Of Pathology", by Guthrie McConnell. Also available from Amazon: A Manual Of Pathology.
Nephritis, Inflammation Of The Kidney
Nephritis, Inflammation Of The Kidney, or Bright's disease is brought about by many conditions, all of which in some way produce an irritation of the kidney by means of the circulation. It follows in the course of poisoning by certain chemicals, such as arsenic, mercury, phosphorus, cantharides, and turpentine; especially in the course of the acute infectious diseases, and also in certain chronic infections, as syphilis and tuberculosis. Nephritis may be acute or chronic and parenchymatous or interstitial, according to whether the changes in the epithelium or in the connective tissue predominate. If both are more or less equally involved the term diffuse is applied.
Acute parenchymatous nephritis is found in the course of the acute infectious fevers, particularly in diphtheria, scarlet fever, and smallpox, and is due to diffusible toxins. The kidneys are usually enlarged, soft, and edematous, the cortex pale and the stellate veins injected. The capsule strips easily, although tense, and the kidney may bulge through the incision. On section, bloody fluid escapes. The cortex is thicker than normal and is much paler than the medulla, which is dark red. The glomeruli may appear as minute red dots. The anemia of the cortex is due to the swelling of the cells, which compress the capillaries. The epithelium is swollen, cloudy, and in many places has become desquamated. This is most marked in the convoluted tubules. In some cases, particularly in scarlet fever, the changes may be most noticeable in the glomeruli, the glomerulonephritis. In this variety the capsular space contains desquamated epithelium from the capsule, red and white blood-cells, granular matter, and an albuminous exudate. The cells may show fatty degeneration. The erythrocytes may be sufficiently numerous to form blood casts.

Fig. 165. - Acute Parenchymatous Nephritis (Catarrhal) (McFarland).
a, Tubule denuded of a large part of its epithelium; b, cells in a condition of degeneration; c, mass of desquamated cells in a tubule.

Fig. 166. - Chronic Glomerulonephritis. X 320 (Dürck).
The capsule fibrillated and thick (5); septa extend inward between the desquamated epithelial cells (3) and leukocytes (4); 2, innermost layer of connective tissue surrounding the greatly diminished tuft (1), which is covered with epithelial cells, the lumen containing leukocytes.
The glomeruli are seldom alone involved, the more common condition being a combination with changes within the tubules.
Ordinarily either of the two preceding varieties terminates in the acute diffuse nephritis, a form in which there are exudative or proliferative changes in the interstitial stroma.
The kidney is larger than normal and may be either dark and congested or pale on account of parenchymatous changes. The cortex is much increased in thickness and shows areas of congestion. The capsule strips easily. The microscopic changes are many. The epithelial cells may be cloudy or swollen, show fatty degeneration, or at times be necrotic. Accompanying these changes there may be a well-marked round-cell infiltration in the connective tissue. There may also be small areas of hemorrhage into the tubules or the capsule of Bowman.
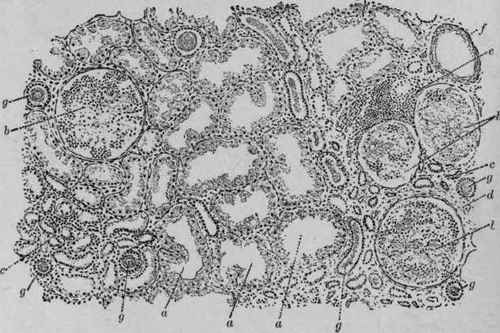
Fig. 167. - Chronic Parenchymatous Nephritis (Kaufmann).
a, Convoluted tubules with cloudy swelling of the epithelium; b, glomeruli, more or less degenerated; c, atrophic tubules; d, sclerotic interstitial tissue; e, round-cell infiltration; f, blood-vessel; g, tube-casts in tubules.
The urine is decreased in amount and at times suppressed, has a high specific gravity (1020-1030), due to the large amount of serum albumen present, is dark in color and contains many casts. Microscopically are seen red and white blood-cells, desquamated epithelium, and tube casts, particularly the epithelial and granular forms.
Continue to:
My Books

