Diseases Of The Bladder
Description
This section is from the book "A Manual Of Pathology", by Guthrie McConnell. Also available from Amazon: A Manual Of Pathology.
Diseases Of The Bladder
Malformations of the bladder are quite common. The most usual form is a lack of union along the anterior median line with failure of closure of the abdominal wall, exstrophy of the bladder. Is usually associated with epispadias, or with division of the clitoris. Occasionally there may be a communication with the rectum or the vagina. Sometimes there is no urethra.
The urachus may remain patulous and urine be discharged at the umbilicus or may be retained in the anterior abdominal wall as a cyst. Diverticula may occur, usually in the anterior wall. The bladder may be completely lacking, the ureters emptying directly into the urethra, or the organ may be divided into two portions by a septum.
Hypertrophy of the bladder may follow any chronic interference to the outflow of urine. The muscular coat of the wall becomes much thickened and the mucous membrane also increases in thickness and is thrown into folds. Indications of chronic inflammation are also usually present.
Dilatation of the bladder may be congenital or acquired. It is due either to obstruction to the escape of urine or to paralysis of the muscular coat of the wall. As a rule, the condition results from long-continued interference with the escape of urine, and is accompanied by a hypertrophy of the walls with thickening of the mucosa. The fibrous bands are prominent and the mucosa in between is pouched. Diverticula are quite frequent. If the dilatation has taken place suddenly, as in paralysis, the vesical walls are very thin. Such a weakening is often accompanied by rupture, with peritonitis.
The bladder may occupy an abdominal position, particularly in women, when there has been some laceration of the perineum. Its walls may prolapse into the vagina, forming a cystocele. At times it may be completely inverted.
Rupture of the bladder may follow severe injury or acute dilatation. The rupture generally occurs at the base and is followed by peritonitis and death. As a result of traumatism the injury commonly occurs near the neck of the bladder and is followed by extravasation of urine into the surrounding tissue, which generally gives rise to a severe phlegmonous cellulitis.
Fistulous communications with the vagina or rectum are not uncommon in women as a result of injuries received during childbirth.
Circulatory Disturbances
Active hyperemia is usually dependent upon infection by some micro-organism or due to the presence in the urine of irritating substances. The mucous membrane is diffusely red.
Passive hyperemia is due to thrombosis of or pressure upon the inferior vena cava. Occurs also in cirrhosis of the liver. The mucous membrane is dark red in color, the vesical veins at the neck of the bladder become distended and varicose, and there is some catarrhal inflammation. Severe hemorrhage may occur from a rupture of one of the varicose veins or the veins may be the seat of thrombosis.
Hemorrhage may be caused by injuries, calculi, malignant disease or result from ruptured varicose veins.
Inflammation
Acute cystitis, inflammation of the bladder, may be due to the presence of pus-producing organisms, to the colon bacillus and the gonococcus, that have gained entrance from the urethra or to the presence of irritating substances within the urine. The infecting agent may have been introduced by the use of unclean instruments in catheterization. The bladder is usually empty or else contains a small amount of cloudy urine that throws down a sediment composed of desquamated epithelium, mucus, pus cells, and bacteria. The mucosa is hyperemic, swollen, and edematous. The process may subside in a short time or it may become pseudomembranous. The inflammation extends into the deeper tissues, necrosis of the epithelium with ulceration takes place, and over these areas is formed a pseudo-membrane. The greater part of the vesical walls may be thus covered.
Phlegmonous cystitis may be a further stage of the above processes, but it usually results from a rupture of the bladder. The vesical walls and the surrounding tissues become infected and are the seat of abscess formation.
Chronic cystitis may follow acute inflammation, but is generally caused by some chronic obstruction to the escape of urine, such as an enlarged prostate or a stricture. As a result of obstruction there is a retention of urine, with subsequent infection. Decomposition follows and the irritating products set up a chronic inflammation. The mucous membrane becomes much thickened and even polypoid, is reddened, and frequently ulcerated. Lime salts may be deposited in the degenerated tissues. The muscular fibers hypertrophy, but they gradually lose their strength and the urine is not discharged. Hemorrhages into the vesical walls are common.
As a result of injuries to the spinal cord the bladder may undergo a rapid dilatation and the walls at the same time have their nutrition interfered with. The urine rapidly collects, undergoes fermentative processes, and causes necrosis of the mucous membrane. This may be followed by perforation with fatal peritonitis and at times gangrene.
Tuberculosis of the bladder is generally secondary to tuberculosis of the epididymis, seminal vesicles, or prostate, or occurs as a descending infection from disease of the kidney. The disease manifests itself in the form of ulcers that are commonly located in the trigone, from which they may extend upward, involving the lower half of the bladder. The involved areas undergo cheesy degeneration and are frequently the seat of a deposit of urinary salts. There is usually a chronic cystitis present. Tuberculosis of the bladder is very much more common in men than in women. Primary tuberculosis is extremely rare and syphilitic ulcers are also very unusual.
Vesical calculi are very frequently encountered. They are composed of substances normally or abnormally present in the urine. They may be present in great numbers, when they are small, like fine particles of sand, or singly as one large stone several centimeters in diameter and weighing as much as 1000 gm. The shape and the general characteristics of the calculi depend upon the material of which they are formed. The stones may be imbedded within the mucosa or they may lie free within the bladder. In the latter case the sides of the stones may be worn smooth by mutual contact. The formation of a stone is generally considered to be due to the precipitation of the various salts about some desquamated epithelium or foreign body. This is accompanied by a coagulation of albuminous material about the calculus and then another layer of mineral salts, giving a distinctly laminated appearance to the stone. Occasionally the nucleus may be a renal calculus that has passed through the ureter. It is usually of a different composition than those formed within the bladder.
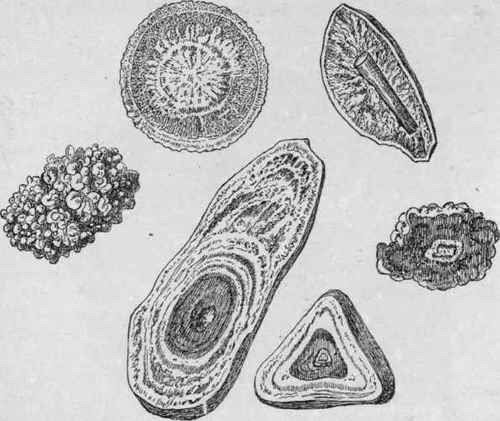
Fig. 172. - Urinary Calculi (Orth).
Showing the nuclei from which they originate, the concentric laminae by which they are formed, the radiating infiltration sometimes observed, and the various smooth and nodular surfaces.
Associated with the formation of calculi is generally a retention of urine.
These stones may be made up of uric acid or urates, of oxalate of lime, of phosphates, of carbonate of lime, or of various organic bodies, as cystin or xanthin.
The characteristics of the various calculi are as follows: 1. Uric acid, are less common in the bladder than in the kidney. Are small, round, hard, slightly granular surface, of a yellowish, reddish, or brownish color. They probably originate within the kidney.
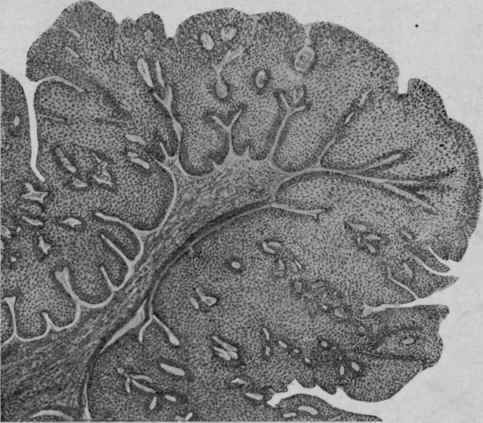
Fig. 173. - Papilloma of the Bladder. X 35 (Ziegler).
Section through a tuft.
2. Urates, of ammonium magnesium, often are covered by earthy phosphates. May be as large as a hen's egg, oval, smooth surface, pale in color, and laminated. If composed entirely of ammonium urate are seldom larger than a pigeon's egg, rounded but also flattened, friable, granular, and dull yellow.
3. Calcium pliosphate, medium-sized, irregular surface, grayish in color, hard and brittle, or soft and crumbling if there is much triple phosphate present. Frequently form about small uric acid calculi.
4. Triple phosphates, large, irregular, grayish, soft, and friable.
5. Carbonate of lime, are rare, are small, white, and chalky.
6. Oxalate of lime, are round, brownish color, surface irregular and nodular, very hard, may be quite large. Are the mulberry calculi.
7. Cystin, unusual, small, oval, brownish or greenish, soft and waxy.
8. Xanthin, very rare, small brownish, smooth surface, and brittle.
Results of the vesical calculi are many. Their presence may cause obstruction to the outflow of urine, with subsequent dilatation of the bladder and its accompanying chronic cystitis. By pressure, atrophy and ulceration of the mucous membrane may take place, with even perforation. Hypertrophy of the vesical walls occurs. There are frequent attempts at micturition, accompanied by straining and tenesmus, with frequent bloody urine. If long continued the obstruction may give rise to bilateral hydronephrosis or pyonephrosis if the infection extends upward.
Sometimes the calculus may become lodged in a pouch of the wall and become completely encapsulated.
Tumors
Polypoid thickenings of the mucosa are quite frequently found in chronic inflammations of the bladder. Papillomata generally appear as small villous outgrowths, covered by epithelium. Are very vascular and may give rise to such considerable hemorrhage that grave or fatal anemia ensues. Occasionally bits of the papillary growths may break off and be passed through the urethra or they may be large enough to cause obstruction. These tumors are benign, but there is a possibility of their becoming malignant. True connective-tissue tumors, particularly sarcoma, are rare. Carcinoma in the form of a squamous epithelioma is an infrequent primary tumor. It occurs as a cauliflower mass that frequently undergoes ulceration. The neighboring organs are generally involved by contiguity. Secondary carcinoma may follow malignant disease of the sexual organs, of the rectum, or of the prostate by direct extension. The bladder is very rarely the seat of a metastatic growth. Cysts very rarely are found.
Continue to:
My Books

