Chapter X. Closure Of Artificial Anus

Description
This section is from the book "Diseases Of The Rectum And Pelvic Colon", by Martin L. Bodkin. Also available from Amazon: Diseases of the rectum and pelvic colon.
Chapter X. Closure Of Artificial Anus
The ordinary methods in vogue for the surgical treatment of these cases include removal of the spur and re-establishment of the normal channel either by resection with subsequent end-to-end Anastasia, lateral Anastasia, or the simple restoration of the skin and mucous membrane coverings.
Pressure Necrosis is produced by variously devised clamps, such as the Uptrend entertainment, Gross's modification of the entertainment and that devised by Ant All these instruments are especially designed to produce pressure necrosis of the spur, which removes sufficient tissue at that point to allow the fecal current to pass unobstructed into the lower segment of the gut.
The instrument devised by Ant has the special advantages of being of little weight and that the shank is bent at right angles to the clamp, permitting it to lie flat upon the abdomen. The jaws of the clamp are defenestrated, about one-half inch broad and about one and one-fourth inches in length. Ant has devised a clamp applicator or forceps to facilitate the application of these clamps. The applicators are not an absolute necessity as the clamp can be pressed upon with the fingers sufficiently to allow it to be applied over the spur without great difficulty. The clamp is allowed to remain in position until it comes away of itself, usually about six to nine days after its application, but this time will be dependent upon the amount and character of the tissue removed. The patient should be kept in bed until the clamp sloughs out, and the pain controlled with morphine, if needed. After the spur has been cut through, the skin and edges of the wound should be freshened and drawn together with catgut or silk sutures.
End-to-end Anastasia Should the preceding operation fail to produce desired results, or be impracticable, end-to-end Anastasia, after resection, is sometimes necessary to establish the normal intestinal channel. An end-to-end Anastasia is performed as follows: The parts are first thoroughly cleansed and the artificial anus closed with continuous catgut sutures to prevent the escape of the bowel contents. The skin about the opening is divided by a semicircular incision and the bowel dissected from its attachments and brought up through the wound. The portion of the bowel which includes the spur is then excised and an end-to-end Anastasia made by means of the Murphy button. A lateral Anastasia or any of the other various operations used for Anastasia of the intestine may be performed at this point
The Ligation Operation. This consists of introducing a ligature through the spur as deeply as possible, which is then tied and allowed to slough through. This operation is not to be recommended for the reason that the needle penetrates the mucous membrane of the bowel and is very apt to carry infection, also that it simply divides or splits the tissue. After the tissue is divided, the skin and the edges of the wound are freshened and drawn together with catgut or silk sutures, as in the clamp operation.
Tittleâs Technique. The plan of operating for the establishment of an artificial anus suggested by Cuttle is intended to facilitate the subsequent closure and appears very practicable. It has been my misfortune in a very protracted case to find that the flaps atrophied and were of no benefit in the attempt at closure of the gut which was later accomplished by the pressure necrosis method described above. However, the operation does not alter the chances for a successful closure by any other method.
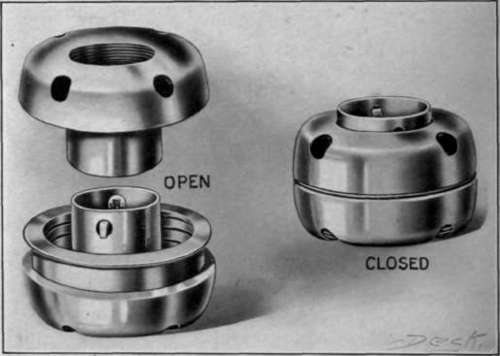
Fig. 26. Morphyâs button.
Tittleâs technique, after following the Madly-Reclus method of operation for inguinal colostomy, is to make an incision through the longitudinal muscular band opposite the dysentery, extending from the superior angle of the wound to half an inch below the supporting glass rod. A transverse incision is then made at the lower end of this incision involving two-thirds of the circumference at the gut. By these incisions the triangular flaps in the upper segment are allowed to curl upward. The straight flap at the lower end of the wound falls downward and inward, partially closing the lower aperture. The fecal evacuations are thus brought out on the surface of the abdomen, preventing escape into the lower segment of the bowel. The lower segment may be opened at any time for the purpose of irrigation and treatment by simply lifting up the transverse Bap. In addition Cuttle claims that no portion of the intestinal wall is sacrificed. When it becomes advisable, the artificial anus can be closed by simply suturing the edges of the T-shaped wound together, without opening the peritoneal cavity.
Continue to:

My Books

