Colostomy. Part 3

Description
This section is from the book "Diseases Of The Rectum And Pelvic Colon", by Martin L. Bodkin. Also available from Amazon: Diseases of the rectum and pelvic colon.
Colostomy. Part 3
These fibers run transversely and may be cut or separated. The external border of the quadratures lumberer and the transverses fascia is then exposed. All bleeding should be controlled and the operating field cleared. The wound is then well retracted and the transverses fascia incised, exposing the sub-serous fat in which the kidney is imbedded and in front of which the colon lies. Caution should be taken in tearing the fat apart with the fingers or blunt instrument so as to avoid wounding the kidney or ureter, should it be misplaced. It is wise to locate the kidney during this dissection, as Bryant claims the colon lies just in front of its lower border.

Fig. 24. Colostomy bag and bandage which may be made for either right or left side.
It may be difficult to find the colon if the gut has collapsed or when the fat is very abundant. Ordinarily the colon is sought at too great a distance from the spine. The only guide needed is the fact that when a piece of the gut is reached without entering the peritoneal cavity it must be the desired colon; but this will be dependent upon whether the dysentery is of normal length. When the gut has been found it should be rolled slightly forward in order to exp6se its posterior surface, and silk ligatures passed through the skin and one-third of the circumference of the gut and then through the skin on the opposite side of the wound. The gut is then incised longitudinally and the loops of the sutures are drawn out through the wound and cut in the middle.
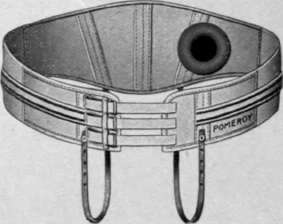
Fig. 25. Inside of the colostomy pad.
The ends are then tied to those passed through the skin of the same side. The gut should be dragged with forceps outside of the wound so as to avoid soiling the field of operation with the escaping feces. Gauze should be packed on each side of the wound before the intestinal incision is made and kept in position until the first discharge of gas and feces. Afterward the intestinal canal should be packed with gauze to prevent further escape. The parts should then be washed, the packing around the gut removed, the skin and intestine brought together with interrupted silk sutures. This technique may be varied by opening the gut immediately as described, or not for several days.
Schnitzelâs, Weir's, Bailey's and Tittleâs methods are variously modified operations devised for permanent colostomy, in which the bowel is dragged beneath the skin or muscles to a variable distance from the original field of operation, making a permanent artificial anus, which is compressed by the intervening tissue, with the idea of controlling the fecal discharge-.
The After-treatment. It sometimes occurs that after the operation for colostomy there will be no movements of the bowels for several days, and it is then necessary to give a laxative or injection of plain water. As a rule, after the first evacuation, the bowels continue to move more often and dressings once or twice a day are necessary. However the intestine accommodates itself to the altered condition after a while, normal evacuations each day become a rule, and the patient often knows beforehand when the bowel is about to empty itself and makes the necessary preparation.
While such patients have no power of controlling the bowel movements, they are able to endure a tolerable existence, often attending to business and social functions without giving evidence of their sad condition. A belt, with a rubber pad having a pneumatic tube border, or to which may be attached a rubber bag into which the contents of the bowel is emptied, may be fitted to prevent the soiling of the clothes by the escape of mucous or fluid fecal matter. A truss with a metal plate controlled by a spring is sometimes used with success.
Continue to:

My Books

