Colostomy. Part 2

Description
This section is from the book "Diseases Of The Rectum And Pelvic Colon", by Martin L. Bodkin. Also available from Amazon: Diseases of the rectum and pelvic colon.
Colostomy. Part 2
Maydayâs operation, as modified by Cuttle, for the establishment of an artificial anus is as follows: An incision three inches long is made through the skin and superficial fascia in a line with the external oblique muscle, beginning at a point one inch above and one and a half inches inside of the anterior superior spine of the ilium.
The fibers of the external and internal oblique muscles are then separated with a dull instrument and drawn apart. The fascia transverses is divided with the knife on a line with Forepartâs ligament. The wound should be thoroughly dried and after all bleeding vessels have been ligated, the sigmoid is dragged out of the wound, a small incision made through the dysentery and a glass rod about one-fourth inch in diameter and four inches long is passed under it. The glass rod should pass beneath the gut and its ends should rest upon either side of the wound. Care should be taken to avoid the blood vessels, when making the incision through the dysentery The lower angle of the wound is then closed by silk or catgut sutures, passed through all its coats in such a manner as to compress the lower leg of the intestinal loop against the glass rod. Several fine chromite catgut sutures are then introduced at the two angles of the wound, including the skin, peritoneum, muscular wall of the gut and then through the peritoneum and skin of the other side. A small pad of chloroform gauze is placed under the projecting rod of each side and along the edges of the wound close to the intestine. The projecting gut should be smeared with sterile Vaseline and covered with gauze. The gut is then dressed with sufficient gauze to protect it from the pressure of the adhesive straps and abdominal bandages. The intestine is never opened at this time.
Should the gut become greatly distended by gas, a trochaic should be inserted to allow its escape. The opening made by the trochaic should be closed at once by Alembertâs sutures and sealed with collocation The patient should be placed in bed and the hips elevated and sufficient morphine given hypo-academically to control vomiting and intestinal peristalsis for ten or twelve hours.
The gut may be opened with safety after the first six hours although it is better to wait two or three days if possible. The opening should be made by an incision through the longitudinal muscular band opposite the dysentery, extending from the superior angle of the wound to one-half inch below the glass rod. A transverse incision is then made at the lower end of this wound, involving two-thirds of the circumference of the gut. These incisions cause the two upper triangular flaps to roll backward, while the segment at the lower incision folds downward and inward, practically closing the lower aperture. The opening of the intestine requires no form of anesthesia The fecal current is thus prevented from entering the lower segment of the sigmoid and no portion of the intestinal wall is sacrificed.
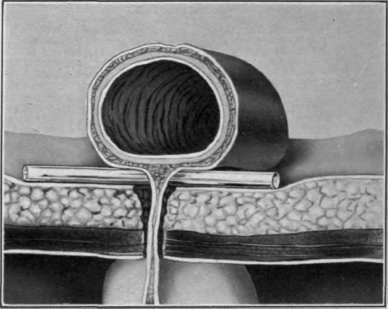
Fig. 22. Colostomy. Cross section Madly-Reclus method.
When the artificial anus is to be closed, the edges of the T wound are sutured together without opening the peritoneal cavity. The lower gut may be irrigated by lifting up the transverse flap. The glass rod should be retained in position with small strips of adhesive plaster for two weeks or longer, as indicated.
When the bowel is distended to such a degree as to cause alarm some surgeons prefer to introduce a Paul's tube. This permits the escape of the gas or fecal matter. The tube is inserted after first placing a circular purse-string suture around the portion of the gut where it is intended to introduce the tube.
The segment of gut is then raised by pulling on a loop of the purse-string suture at one end and on the ends of the suture below. Then a crucial incision is made into the bowel within the area surrounded by the purse-string suture. The Paul's tube has a double flange at the end, which is intended to fit inside the gut and between which the purse-string suture is tied tightly so as to prevent its slipping outward. A rubber drainage tube should be attached to the distal end of the Paul's tube and the contents of the bowel allowed to drain off into the vessel provided for that purpose.
This idea has proven no better to me than the cannula, when we consider the apparent safety which almost invariably follows the use of the trochaic and cannula with immediate sutures. In some instances, as pointed out by Sir Charles Ball, neither of these efforts to relieve the distention are of any benefit, as there will be no discharge of gas or fecal matter for several days. It is probable that in these cases the traumatize to the bowel while operating produces a temporary intestinal paralysis; that the extreme distention has caused a kinking above the field of operation; or, that a reverse peristalsis has been instituted as the result of the operation.
Transverse Colostomy is the making of an artificial anus in part of the transverse colon. In this operation the bowel is attached to the external abdominal wall just above the umbilicus. The technique of the operation is about the same as that employed in the left inguinal colostomy, excepting that the site of the artificial anus is in the median line. The dysentery of the transverse colon ordinarily is not so long as the sigmoid dysentery, and a providential of the gut is not so liable to happen.
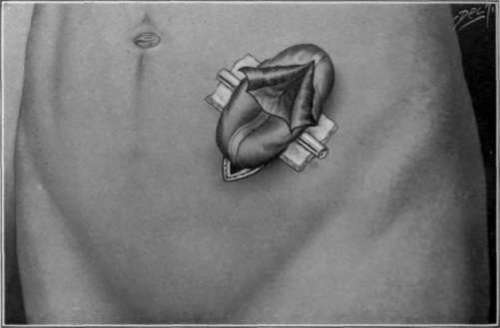
Fig. 23. Tittleâs incision for opening the gut for temporary inguinal colostomy.
Left Lumbar Colostomy is an operation almost obsolete in modern surgery on account of the ease with which inguinal colostomy can be performed with the experience, judgment, and facilities afforded the average surgeon. The technique of the operation is as follows: The patient is placed upon the right side, turned somewhat on his face and held in this position with a sand bag or pillow under the hips. An incision is begun one and a half inches back of the anterior superior spine of the ilium just below the border of the last rib. This incision should extend downward and forward for about four and a half or five inches, parallel with the crest of the ilium. The fibers of the external oblique and dissimulates Doris muscles should be separated and held apart with broad detractors The fibers of the internal oblique are then separated in the same manner by blunt dissection, thus exposing the lumbar fascia
Continue to:

My Books

