Cancer Of The Larynx
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Cancer Of The Larynx
Epidemiology. Incidence
Men | Women |
5,000 new cases each year | 500 new cases each year |
1.98 of male cancer incidence | 0.2% of female cancer incidence |
Mortality
Men | Women |
2,100 deaths each year | 200 deaths each year |
1.4% of male cancer mortality | 0.2% of female cancer mortality |
Rates And Ratios
Male | Female | Sex ratio | |
Incidence per 100,000 | 5.5 | 0.6 | 9 to 1 |
Mortality per 100,000 | 2.4 | 0.2 | 12 to 1 |
Trend Last Ten Years
Male | Female | |
Incidence | - | - |
Mortality | - | - |
Age
Male | Female | |
Significant increase beyond age | 45 | - |
Over 75% of cases occur between ages | 55-80 | 50-75 |
Etiology
The etiologic or predisposing factors in cancer of the larynx are essentially the same as those described for mouth cancer: namely, the use of tobacco and heavy consumption of alcohol.
Pathology
Virtually all cancer of the larynx is epidermoid carcinoma. Leukoplakia of the vocal cords may also occur and is believed to harbor a significant potential for subsequent cancer development.
Classification
For descriptive purposes the larynx is usually subdivided anatomically into the intrinsic and extrinsic larynx (Fig. 40).
The two sites behave quite differently from the standpoint of clinical manifestations and prognosis.
Clinical Manifestations Of Cancer Of The Larynx. Localized Lesion Intrinsic Larynx
Symptoms
1. May be none. Lesions may be found on routine examination. This is quite rare, however.
2. Vague sense of irritation and "tickle" in the throat.
3. Change in voice. Alteration of the quality, timbre, or resonance.
4. Hoarseness.
Signs
1. May present as an indurated, ulcerated plaque or as granular papillary lesions on the vocal cord.
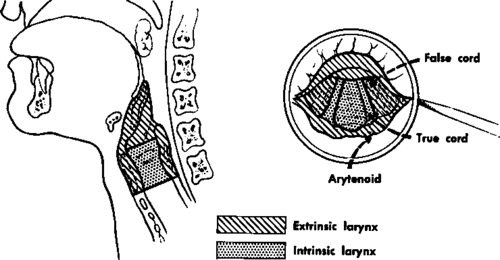
Fig. 40. Sagittal section (left) and mirror view (right) of the intrinsic and extrinsic larynx.
2. Cervical node metastasis uncommon; almost never the first sign.
3. Usually close to free edge of the anterior two thirds of the vocal cord.
Extrinsic Larynx Symptoms
1. Rarely none. Lesions may be found on routine examination, or a metastatic node may direct attention to the area.
2. Throat discomfort, fullness, pain, or soreness, especially on swallowing- usually quite vague in character.
3. Dysphagia.
4. Hoarseness or other voice change are late symptoms. Signs
1. A fungating, papillary lesion, often fairly sizeable when first seen; considerable associated edema may be noted.
2. Metastatic node or nodes may appear early.
Advanced Lesion
The symptoms listed for the local lesion become progressively more persistent, severe, and disabling.
The precise nature and sequence of symptoms and signs associated with advanced disease depend on the exact location of the lesion but, in general, do not differ greatly from those described in the preceding section with regard to advanced mouth cancer.
Steps In The Diagnosis And Initial Management Of The Larynx Cancer Suspect
1. Insist on adequate visualization of the intrinsic and extrinsic larynx in all patients
(a) With recurrent or persistent throat soreness or discomfort, voice change or difficulty swallowing, especially if they smoke and drink heavily.
(b) With cervical adenopathy of unknown etiology. This may be accomplished by means of
(a) Indirect laryngoscopy with the use of a headlight and laryngeal mirror as described in Chapter II (The Cancer Detection Examination). Often it is possible to do this with relative ease. Occasionally topical anesthesia may be required to ensure good visualization.
(b) Direct laryngoscopy by someone experienced in this exacting technique. This may be required for adequate visualization and biopsy, especially of lesions of the intrinsic larynx and postcricoid lesions.
2. After an apparently negative initial examination, a brief trial of local and antibiotic therapy is reasonable provided adequate follow-ups of the patient are maintained. Re-examination and further evaluation should be insisted upon if complaints persist.
3. Biopsy any suspicious lesions encountered in the course of examination.
(a) The extrinsic larynx can usually be biopsied by means of a curved forceps guided by a laryngeal mirror.
(b) The intrinsic larynx usually requires direct laryngoscopy for biopsy,
4. Do not biopsy any cervical lymph nodes until a careful search for a primary lesion in the head and neck region (and elsewhere) has proved negative.
5. An x-ray film of the chest should be made to rule out the presence of primary or metastatic lesions there. X-ray studies of the soft tissues of the neck and the larynx are done by some workers to evaluate the extent of the lesion and to gauge its operability.
6. Patients who have leukoplakia of the vocal cords or elsewhere in the head and neck region, as well as those who have symptoms clearly related to long-term heavy smoking, should be warned of the possible consequence of continuing the habit. Admonitions regarding heavy drinking are also warranted for any individual with laryngeal complaint or findings.
Continue to:
My Books

