Chapter IV. Head And Neck
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Chapter IV. Head And Neck
Primary cancer of the head and neck region occurs mainly in the following sites:
1. Mouth (hps, gums, buccal mucosa, palate, tongue, floor of the mouth, tonsils, and pharynx)
2. Larynx
3. Thyroid gland
The malignant lymphomas (see Chapter IX (Colon And Rectum), p. 266) may present in the head and neck area first; occasionally this may be the only evidence of the disease anywhere in the body. This subject will be dealt with in Chapter IX.
Metastatic cancer which has spread from lesions in the chest, abdomen, and elsewhere may, of course, involve cervical lymph nodes and be confused initially with primary head and neck tumors.
Numerically, cancer of the head and neck region is of rather modest importance. However, from a number of other standpoints, knowledge of the malignant lesions of the head and neck area is of genuine significance.
1. The lesions by and large are readily accessible to simple inspection and palpation.
2. The relationship of curability to stage of disease is probably more obvious and well established here than in any other part of the body at present. The need for detecting disease in a localized state is therefore particularly important.
3. A sizable proportion of the cancer in this region is related to extrinsic factors and therefore susceptible to preventive measures.
A. As a result of lack of knowledge or misconceptions, a number of mistakes are commonly made in the handling of such cases. These errors are relatively easy to avoid, and the initial management of head and neck lesions can be carried out correctly in the physician's office.
5. Great controversy and confusion have surrounded the recommended management of nodular goiters. Since this is a relatively common problem, it is important that the physician have the facts and issues clearly in mind so that he can make appropriate decisions.
Screening Presumably Well Adults For Head And Neck Cancer-Detection
Only inspection (including indirect laryngoscopy) and palpation have been found to be useful in the routine survey of presumably healthy adults for cancer in the head and neck regions. Laboratory, x-ray, and other detection methods have not proved to be generally useful or practical in this area.
The particular techniques of inspection and palpation are described in Chapter II (The Cancer Detection Examination). This chapter is confined to the clinical manifestations of the common cancers of the head and neck region and the methods found useful in their diagnosis.
Relative Frequency Of Head And Neck Cancers
Before taking up the individual sites in sequence, it is helpful in achieving some perspective to consider the relative frequency of the various types of cancer as they occur in the head and neck region.
If the total amount of head and neck cancer is regarded as 100%, the individual sites are affected as shown in Fig. 37.
Also, since the lymph nodes are often involved by palpable metastatic disease, which, rather commonly, may be the only clue to internal disease, some knowledge of the lymphatic drainage of the head and neck region is important (Fig. 38). The precise location of the nodal involvement may help to focus attention on a specific internal site.
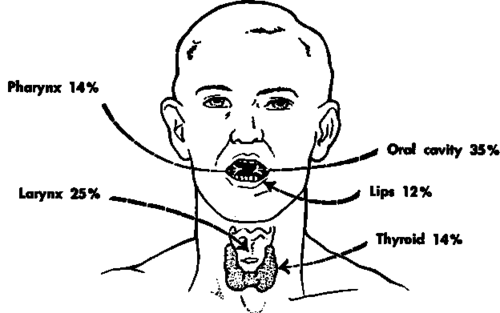
Fig. 37. Distribution of cancer in the head and neck region, excluding skin.
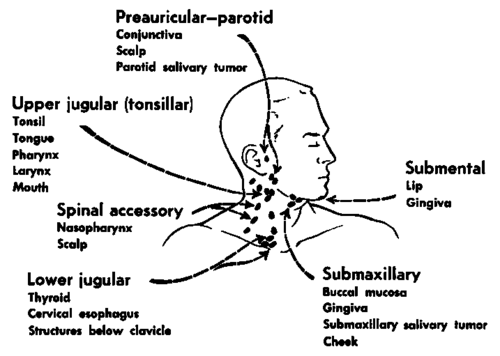
Fig. 38. Areas of drainage to cervical lymph nodes. (Based on data from exhibit of Dr. H. VV. Farr, 1961.).
Continue to:
My Books

