Clinical Manifestations Of Oral Cancer (Lips, Gums, Buccal Mucosa, Palate, Tongue, Floor Of The Mouth, Tonsils, And Pharynx)
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Clinical Manifestations Of Oral Cancer (Lips, Gums, Buccal Mucosa, Palate, Tongue, Floor Of The Mouth, Tonsils, And Pharynx)
Localized Lesion Symptoms
1. May be none, especially if the lesion involves relatively insensitive structures with rather limited functional requirement.
2. Often the patient sees the lesion in the mirror or feels an abnormality with his tongue.
3. Pain and discharge are relatively late symptoms and usually reflect secondary infection.
4. Difficulty with dentures, e.g., irritation from contact with lesions.
5. Bleeding.
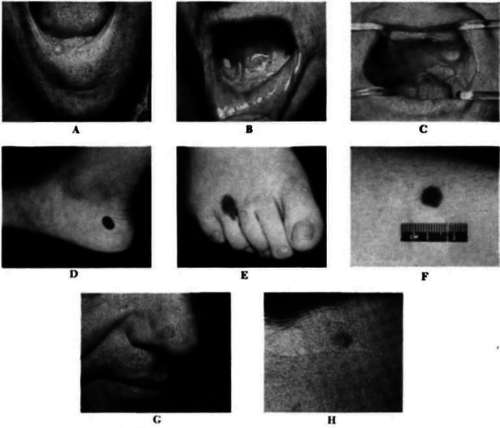
Plate 1
A, Squamous carcinoma of the lower lip. B, Squamous carcinoma of the floor of the mouth, light, and leukoplakia, left. C, Carcinoma of the soft palate. D, Compound nevus. E, Junctional nevus. F, Blue nevus. G, Basal cell carcinoma of the nose. H, Basal cell carcinoma of the forehead.
Signs
1. A small indurated and/or ulcerated coarsely granular lesion with a tendency toward rolling of the edges. Peripheral extension and infiltration beyond the bounds of the visible lesion may be palpable with the examining finger.
2. Leukoplakia is often associated with the lesion.
3. Sometimes, despite a very small primary lesion, cervical node involvement by metastasis is demonstrable. This, in fact, may be the first clue as to the presence of the cancer.
Advanced Lesion Symptoms
1. Pain usually present. May be due to:
(a) Secondary infection.
(b) Bone invasion.
(c) Nerve involvement (cervical nerve roots). Usually the result of a combination of all three.
2. Salivation and drooling due to hypersecretion, secondary infection, and inability to swallow properly as a result of pain or obstruction.
3. Foul breath due to necrosis and secondary infection of tumor.
4. Earaclie or fullness.
5. Symptoms secondary to bulky disease in the neck and posteriorly
(a) Bespiratory obstruction with stridor, dyspnea, etc.
(b) Pharyngeal and esophageal obstruction with dysphagia.
(c) Hoarseness.
Signs
1. The primary tumor may reach great size, especially if situated posteriorly where expansion is possible.
2. Secondary infection and necrosis usually is present.
3. Hemorrhage may occur.
4. Invasion by the tumor of adjacent soft tissue, bone, sinus cavities, etc. is often obvious.
5. Evidence of nerve involvement (recurrent laryngeal, vagal, hypoglossal, sympathetic).
6. Metastatic node involvement, unilateral or bilateral, often of great bulk, is usually present.
7. Evidence of weight loss, cachexia, anemia, etc. due to effects of tumor proper or of near-starvation.
8. Occasionally distant metastasis, e.g., to the lungs, liver, bones, etc. occurs but disease usually advances by contiguous local invasion.
Continue to:
My Books

