Steps In The Diagnosis And Initial Management Of The Mouth Cancer Suspect
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Steps In The Diagnosis And Initial Management Of The Mouth Cancer Suspect
1. Biopsy any suspicious lesion in the mouth. This may be done in one of three ways (Fig. 39). In performing incisional biopsy by whatever technique, it is important to obtain a piece of adjacent normal tissue at the border of the lesion to determine extent of invasion. Avoid necrotic material and trauma which crushes the specimen. For lesions of the oral cavity, local anesthesia is best provided by a combination of topical Ponto-caine or Xylocaine followed by infiltration with 1% procaine and judicious use of Adrenalin when tolerated by the patient. Sutures are rarely necessary, and bleeding is normally not a problem.
2. Two weeks or less should be allowed for a therapeutic trial of antibiotics, mouthwashes, etc. Even this brief period should not be allowed if the lesion is obviously suspicious or the patient cannot be counted upon to return for follow-up. Lesions persisting beyond this arbitrary time limit must be biopsied.
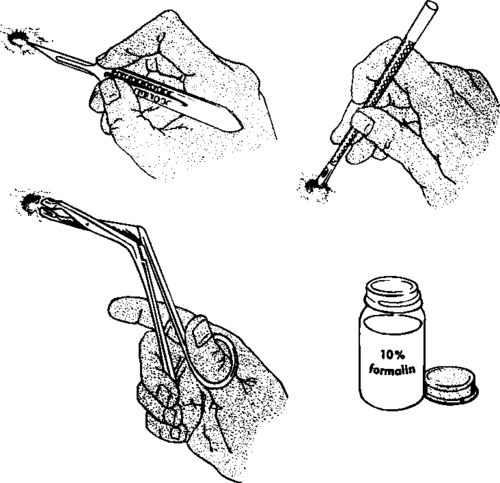
Fig. 39. Incisional biopsy by scalpel, Martin punch, and biting forceps.
Dental extractions of presumably infected teeth to evaluate the effects on cervical adenopathy should be done only after careful exclusion of cancer. Otherwise, not only may this lead to weeks of delay in diagnosis, but also spread of the mouth cancer may be abetted and subsequent therapy impeded.
3. Metastatic neck nodes should seldom be biopsied.
4. Occasionally, of course, the only hint of cancer in the head and neck region is the presence of one or more suspicious lymph nodes. These should be the signal for an intensive search for the primary lesion. The map of the lymphatic pathways of the head and neck (Fig. 38, p. 94) indicates the varying significance of such nodes according to location. A clue may be provided as to where to look first. In any event, the oral cavity, pharynx, larynx, nasopharynx, sinuses, thyroid, and scalp should be diligently surveyed.
The occult primary lesion thus uncovered should then be subjected to biopsy in the manner described under point 1. The metastatic lesion should not be biopsied, except as a last resort.
Failure to follow this sequence when confronted by a patient with a "lump in the neck" may result in serious errors in management. Biopsying a metastatic neck node without first searching for the primary lesion has been compared to excising an axillary node in a woman without examining her breast. Such a policy may delay diagnosis and treatment and unnecessarily scar an operative field.
If no primary lesion can be found in the head and neck region or elsewhere to account for the enlarged nodes, biopsy may be carried out since the lesion may represent Hodgkin's disease, sarcoidosis, tuberculosis, etc.
5. Blood serology should be done in the case of suspicious tongue lesions since up to 20% of patients with cancer of the tongue may have a positive test. Actually, however, this is of little assistance in the differential diagnosis since cancer and syphilitic glossitis (and other syphilitic lesions) may co-exist, and only biopsy will distinguish the two.
6. X-ray examinations may include views of the following:
(a) Chest. It is particularly important that a chest film be taken before biopsy is done in patients presenting only with clinically suspicious nodes in the neck since the primary lesion may be in the intrathoracic organs. It may occasionally reveal unsuspected pulmonary metastases from head and neck lesions, too. Finally, the presence of mediastinal widening, hilar adenopathy, etc. may suggest the diagnosis of Hodgkin's disease or one of the other malignant lymphomas.
(b) Maxilla, mandible, and sinuses. This is done primarily to evaluate the possibility of bone invasion or spread from mouth cancers (especially those of the gums and palate).
7. The presence of other primary lesions in the adjacent respiratory passages should be ruled out since their frequency is increased several-fold in the presence of mouth cancer. Any patient with well-established leukoplakia should be singled out for special attention.
1. He should be re-examined regularly, perhaps at six-month intervals, in order to detect the appearance of superimposed cancer.
2. He should be informed of the definite relationships of leukoplakia to smoking (and, to a lesser extent, to heavy drinking) and of the very real risk he is taking if he continues to indulge in both. Absolute prohibition of smoking and sharp reduction in alcoholic consumption is indicated in most instances.
Continue to:
My Books

