Malignant Lymphomas
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Malignant Lymphomas
The term malignant lymphoma is actually a rather arbitrary generic grouping of several diseases which appear to have as a common denominator the neoplastic growth of lympliatic and/or reticuloendothelial tissues.
1. The term is capable of almost infinite divisions and subdivisions, and the resulting nomenclature can lead to great confusion. For practical purposes it is perhaps best to limit the breakdown to the following three categories:
(a) Hodgkin's disease
(b) Lymphosarcoma
(c) Reticulum cell sarcoma
2. Few diseases have a greater capacity than the lymphomas to involve so many body organs or systems and present such a variety of clinical syndromes.
3. Contrary to some opinion, there is evidence that the lymphomas are not necessarily systemic diseases from their onset. On occasion they may be unicentric or localized, and thus the timing and aggressiveness of therapy may be quite important under these circumstances.
Epidemiology. Incidence
Men | Women |
10,200 new cases each year | 7,000 new cases each year |
4% of male cancer incidence | 2.9% of female cancer incidence |
Mortality
Men | Women |
8,000 deaths each year | 5,650 deaths each year |
5.5% of male cancer mortality | 4.6% of female cancer mortality |
Rates And Ratios
Male | Female | Sex ratio | |
Incidence per 100,000 | 11.3 | 7.6 | 1.5 to 1 |
Mortality per 100,000 | 8.1 | 5.7 | 1.4 to 1 |
Age
Male | Female | |
Significant increases beyond ages | 25+ | 25-40 |
Over 75% of cases occur between ages | 40-74 | 45-80 |
Trend Last Ten Years
Definite, though relatively small, over-all increases are apparent for both men and women.
Etiology
The etiology of the malignant lymphomas is completely unknown.
There has been much speculation and theorizing in recent years about the possibility of an infectious agent (e.g., virus, tubercle, brucella, fungus, and other organisms) producing a granulomatous reaction and thus giving rise to the lymphomas. Proof has been notably lacking to date, however, and the majority opinion remains that the lymphomas are true neoplasms of unknown etiology.
It is worth noting that, unlike leukemia, there appears to be no evidence of a relationship between exposure to ionizing radiation and subsequent development of the malignant lymphomas.
Pathology
The diagnosis of the malignant lymphomas requires microscopic review of a representative tissue section by a competent pathologist.
It is not our intention to discuss the very complicated and sometimes controversial pathology of the malignant lymphomas. Suffice it to say that the disease is characterized by the neoplastic proliferation of lymphoid and/or reticulum tissue in the lymph nodes, spleen, and other organs.
For ordinary clinical purposes it is probably wise to confine the malignant lymphomas to the three major divisions mentioned previously (Hodgkin's disease, lymphosarcoma, and reticulum cell sarcomas) and leave it to the pathologist to assign the patient to a more specific category.
However, a few practical points are worth noting about the sometimes bewildering pathology of the malignant lymphomas.
1. The initial lymph node biopsy may sometimes be interpreted as nonspecific lymphadenitis or granulomatous reactions. Weeks or months later a specific microscopic diagnosis of one of the lymphomas may be possible from clinically similar nodes.
2. In the same individual the disease may show considerable variation in its microscopic pattern:
(a) Occasionally in sections taken from different parts of the same node
(b) More commonly in different nodes taken from different parts of the body
(c) In serial biopsies taken from the same or different locations over a period of time
3. In general, the foregoing are all variations within a specific type of lymphoma (e.g., so-called Hodgkin's granuloma, paragranuloma, and sarcoma). Occasionally, however, the differences may be so striking that it may almost appear that two types of lymphoma coexist in the same patient or that there has been a transmutation in type during the course of the illness. As a rule, the coexistence of two different lymphomas in the same person is exceedingly rare, and the prevailing opinion is that change in the type of an established lymphoma does not occur. In view of the foregoing, it is not surprising that different pathologists may render different lymphomatosis diagnoses when confronted with the same material. Fortunately, certain general principles of prognosis and therapy can usually be applied to the over-all grouping of the malignant lymphomas.
Clinical Classification
It is helpful to think of the malignant lymphomas in terms of the broad clinical classification proposed by Diamond.
Class I Disease limited clinically to a single locus (unifocal, unicentric origin); no constitutional symptoms or signs (i.e., fever, night sweats, pruritus, weight loss, anemia, fatigue)
Class II Disease limited regionally (regional anatomic distribution (e.g., all apparent disease above the diaphragm or all apparent disease below the diaphragm), with or without constitutional symptoms and signs
Class III Generalized (universal) disease with constitutional symptoms and signs
Such a classification is of particular usefulness in choosing therapy and estimating prognosis, but it also serves to underscore an important concept regarding the natural history of the disease.
It is, of course, possible to consider the clinical manifestations of each of the malignant lymphomas separately. However, they share so many common features that differentiation between the individual subdivisions is often not possible on clinical grounds alone but rather must await the pathologist's report. In this discussion, Hodgkin's disease, lymphosarcoma, and reticulum cell sarcoma will be treated as one entity from the standpoint of symptoms, signs, and diagnostic measures.
SCREENING PRESUMABLY WELL ADULTS FOR THE PRESENCE OF THE LYMPHOMAS-DETECTION
Two parts of the routine cancer detection examination may provide the first clue to the presence of one of the lymphomas in an apparently healthy adult. 1. Physical examination. The presence and persistence of otherwise unexplained adenopathy should always raise the question of the lymphomas.
A

B

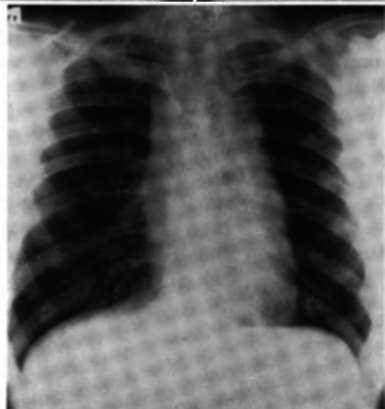
C
Fig. 82. A, Hodgkin's disease. There is a widening of the superior mediastinum generally, especially to the right. Note that the aortic knob is obscured by the mediastinal tumor.
B, Hodgkin's disease, same patient, after therapy. Note the dimunition in the width of the superior mediastinum soon after x-ray therapy. Slight superior mediastinal widening still persists on the right.
C, Lymphosarcoma. Massive mediastinal widening obscuring all the vascular structures is present.
The manner in which this may present will be detailed below. The presence of splenomegaly and/or hepatomegaly may also raise this suspicion. 2. X-ray film of the chest. Not uncommonly the first manifestation of one of the lymphomas, especially Hodgkin's disease, is the finding of mediastinal widening, adenopathy, or other intrathoracic abnormality on a routine chest film (Fig. 82). As in virtually all types of cancer, the first clue to the presence of the disease may be latent or subclinical symptoms not regarded as significant by the patient (e.g., fatigue, pruritus, low-grade fever, nightsweats, etc.) elicited in a carefully taken history.
Occasionally, of course, the finding of anemia as reflected in the routine blood count may be encountered in the course of the basic examination. This is seldom the only finding in the case of the lymphomas, however. It more commonly serves to bolster a suspicion raised by the physical examination or findings on the chest film.
Clinical Features Of The Malignant Lymphomas-Diagnosis. Localized Lesion
It is not common for the malignant lympohmas to present as a truly localized lesion. Nevertheless, as noted previously, it would appear that a localized lesion can occur and, when it does, it may have important implications insofar as prognosis and treatment are concerned.
This localization may occur in virtually any tissue, organ, or site in the body. Usually it is an enlargement of a single node or groups of nodes that signifies the presence of the disease. Quite commonly, apparently localized disease will, on more careful evaluation, prove to be only part of a more generalized process.
Enlargement of a cervical lymph node or restricted group of nodes is probably the most common type of localized malignant lymphoma. Isolated axillary, inguinal, and other adenopathy may occur also. On other occasions the lympho-matous process may appear to be confined to a single portion of the gastrointestinal tract (especially the stomach and small intestine), the lungs, the bones, the spleen, the tonsil, or other tissues.
The symptoms and signs produced by the disease reflect the site of localization. Most commonly, painless lymphadenopathy is the only finding. There are no constitutional or systemic manifestations of truly localized disease.
Continue to:
My Books

