Classification Of Bladder Tumors
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Classification Of Bladder Tumors
There are many methods of classifying bladder tumors. A relatively uncomplicated and satisfactory one is as follows:
1. Papilloma-a papillary lesion that is microscopically benign.
2. Carcinoma-a microscopically malignant lesion that grossly may be papillary or nonpapillary.
Bladder carcinoma, whether it is papillary or nonpapillary, is classified further for prognostic purposes in a manner somewhat analogous to that utilized for the rectum and colon:
1. By grade according to the degree of cellular differentiation (Grades I, II, III, and IV).
2. By stage according to the depth of invasion of the bladder wall and metastatic spread (Fig. 79).
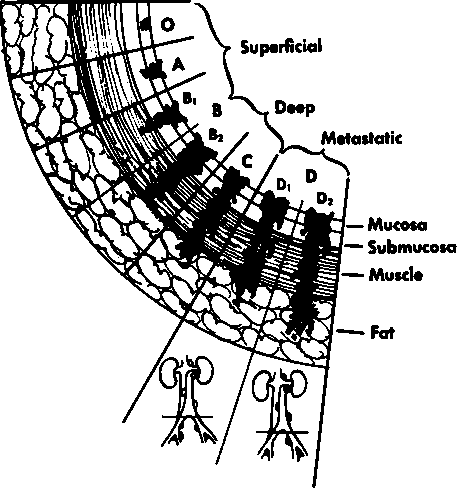
Stage O | Growth limited to the macosa |
Stage A | Growth limited to the mucosa and submucota |
Stage B | Muscle Invasion |
Stage B1 | Superficial to the halfway level |
Stage B2 | Deep |
Stage C | Invasion of the perivesical fat |
Stage D | Metastasis |
Stage D1 | Local to the pelvis |
Stage D2 | Beyond |
Fig. 79. Staging of bladder cancer. (Based on data from Marshall, V. F.: Current Clinical Problems Regarding Bladder Tumors, Cancer 9:543, 1956.).
Such a combined method of classification, reflecting both differentiation and invasion, is quite helpful in evaluating the actual state of the disease, choosing therapy, and estimating prognosis. Classification of this sort is usually possible from an adequate cystoscopic biopsy, careful bimanual examination, and the findings on intravenous pyelograms.
Histologic Type
From 90 to 95% of all malignant bladder tumors arise from the lining transitional epithelium of the bladder and are classified as epidermoid carcinoma, or, more familiarly, transitional cell carcinoma.
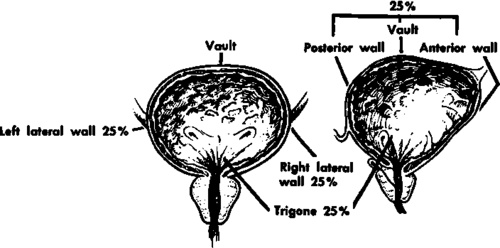
Fig. 80. Location of cancers of the bladder.
Location
Cancers of the bladder show certain sites of predilection (Fig. 80).
1. About 25 to 30% occur in the region of the trigone.
2. About 25% occur on each lateral wall of the bladder.
3. The remaining 20 to 25% occur in the vault or the anterior and posterior walls of the bladder.
Such a "map" of the bladder lesoins emphasizes the fact that even localized bladder cancer
1. May cause ureteral obstruction on one or both sides.
2. May be difficult to treat by conservative surgery because of its frequent involvement of strategic and vital structures.
Also emphasized by the location of most of the lesions is the possible role of a urine-borne carcinogen.
Single Or Multiple
Approximately 20% of all bladder papillomas or cancers are multiple.
Screening Presumably Well Adults For Bladder Cancer-Detection
In taking the history, the physician may come across leads which might alert him to the possibility of bladder cancer.
1. Environmental, occupational, or other exposure to a carcinogen, even years in the past
2. History of a bladder papilloma or polyp at any time in the past
3. Minimal and subclinical genitourinary symptoms, almost unnoticed by the patient
The urinalysis is the only laboratory test that has proved helpful in screening for bladder cancer. Gross or microscopic hematuria must always be regarded with suspicion.
Physical examination is seldom helpful, especially in the localized lesion.
Cytologic examination of the urinary sediment is not advised for routine screening purpose unless there is particular reason to believe that the person is at high risk for bladder cancer.
Continue to:
My Books

