Steps In The Diagnosis And Initial Management Of The Cervical Cancer Suspect
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Steps In The Diagnosis And Initial Management Of The Cervical Cancer Suspect
The physician may be confronted by one of two typical situations in which he has to rule out the presence of cancer:
1. The cervix may have appeared perfectly normal or benign, but the cytologic report on the smears comes back suspicious or positive for epidermoid cancer.
2. The cervix may have aroused suspicion because of its clinical appearance and/or a positive iodine test. The cytologic report may have come back suspicious, positive, or negative.
The management of these two situations will be considered separately since this is the way they tend to occur in the doctor's office. There is considerable overlapping, however, and often the issues are not so clear-cut as they are presented here.
Management Of The Patient With A Suspicious Or Positive Smear
1. Re-examine the patient. Do another pelvic examination and repeat the vaginal and cervical smears. Occasionally a small lesion can be seen on this second visit.
2. Repeat the iodine stain of the cervix and observe for nonstaining areas.
3. Biopsy. In general, the recommendation is to perform a biopsy on any patient who shows a single positive or suspicious smear. Certainly this is true if the smear was positive. However, if the initial smear was only suspicious or somewhat atypical and the patient is very reliable and cooperative, it may be possible to wait and see what the second smear shows before proceeding with biopsy. The recommended biopsies are:
(a) The four-point biopsy-done as shown in Fig. 55.
(b) The endocervical biopsy-done as shown in Fig. 56.
If the iodine test has proved abnormal and thus indicated a suspicious area, this area should, of course, be carefully biopsied. Usually this is adequately encompassed by the four-point and/or endocervical biopsy.
This type of comprehensive biopsy survey is almost certain to detect a carcinoma in situ lesion if one is present.
Occasionally the initial biopsies may be genuinely negative even in the face of very strong prior cytologic evidence of cancer. Under these circumstances the usual assumption is that the in situ lesion may have been so superficial and localized that the mere trauma of taking the cervical smear removed it. Also, if the interval between smear and biopsy were long enough, the lesion may have regressed spontaneously. One should always remember to recheck the vagina, since an occult carcinoma here may yield smears positive for epidermoid cancer even though the cervix is normal. 4. If repeated cytology is found to be:
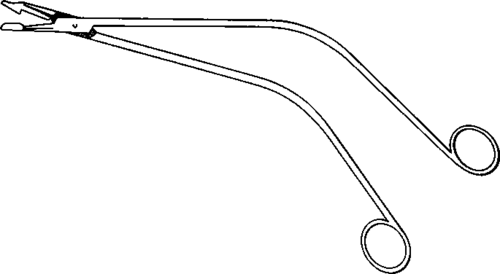
Fig. 54. Schubert cervical biopsy forceps.
(a) Negative or abnormal-but-benign. Repeat the pelvic examination and take smears at an interval of three to six months and then yearly thereafter.
(b) Suspicious. If biopsy has not already been accomplished, it certainly should be done now. If biopsy has been clone, management is based upon the report of this material, not the cytology.
(1)If the biopsy is negative, the patient may be followed by means of smears at three to six month intervals for an indefinite period.
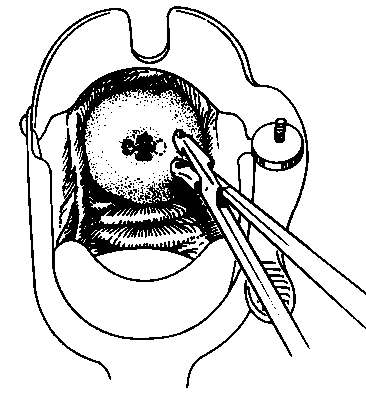
After painting the cervix with 7% Iodine, introduce the biopsy forceps with the flat surface against the endocervical wall. Open the forceps gently, exerting pressure against the area of the cervix to be biopsied) then close the forceps.
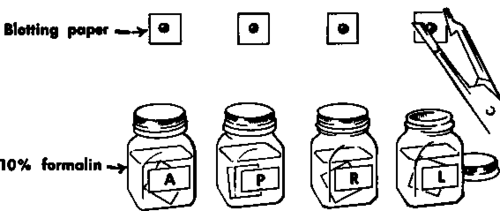
Place the specimen on blotting paper.
Immerse in 10% forma-Iin. The letters A, P, H, and L on the bottles refer to the source of the biopsy: anterior, posterior, right, and left.
Insert a tampon to control bleeding, and instruct the patient to remove It in twelve to twenty-four hours.
Fig. 55. Technique of four-point biopsy of the cervix.

Insert the closed punch biopsy forceps into the endocervical canal. Gently spread the forceps and close again to obtain biopsy specimen. For biopsy of the opposite endocervical surface, reintroduce the forceps in the reverse position and repeat the procedure.
Place specimen on blotting paper.
Immerse in 10% formalin.
Insert a tampon to control bleeding, and instruct the patient to remove it In twelve to twenty-four hours.
Fig. 56. Technique of endocervical biopsy.
(2) If the biopsy is positive, the patient should be handled in accordance with the pathologist's description of the lesion, i.e., in situ or invasive carcinoma (see below). 5. If repeat cytology is found to be positive. In most instances the appropriate biopsies will confirm the presence of cancer when the cytology is twice positive. Management depends on whether the disease is thought to be intraepithelial (in situ) or invasive on the basis of its histologic characteristics. Occasionally, of course, the cytology will be twice positive and the biopsies negative. This dilemma must be resolved according to the particular circumstances of the case. Usually this calls for hospitalization with a diagnostic dilatation and curettage and conization. Occasionally it may be possible to observe such a patient with safety months or years on a strict program of re-examination every one to three months.
Management Of The Patient With The Clinically Auspicious Lesion
Obviously, this covers a vast area of clinical suspicion, from that aroused by the patient with a relatively minor cervical erosion to that of Stage IV advanced disease.
Certain steps can be outlined, however.
1. Biopsy the lesion or suspicious area at the time of the first visit. In addition, the four-point and endocervical biopsies may be done for the additional information they may provide.
2. Smears. One should never rely upon the cervical smear alone to pass judgment on a suspicious lesion. As long as one is aware of this precept, there is no harm in doing smears under such circumstances, but they seldom can be counted upon to provide additional information. Cytology should never be regarded as a substitute for biopsy in the evaluation of the suspicious lesion.
3. When the biopsy report is available:
(a) If the report is negative or benign, the usual local corrective measures can be instituted. The patient should be followed, however, and recalled at three- to six-month intervals for repeat smears and/or biopsy, depending on the response of the lesion.
(b) If the report is positive, then definitive treatment is undertaken, the type and extent depending upon the type of lesion described histologically and felt clinically.
(c) In situ cancer is handled in a manner to be outlined below.
(d) Invasive cancer requires conventional surgical or radiotherapeutic or combined management for cure or palliation.
4. When the biopsy shows invasive cancer, other diagnostic steps may include:
(a) Careful repeat pelvic examination to assign the lesion to one of the stages of the international classifications and to decide upon therapy.
(b) Intravenous or retrograde pyelograms to rule out urinary tract obstruction.
(c) Sigmoidoscopy and barium enema on indication to rule out lower bowel invasion.
Management Of The Patient With In Situ Cancer Of The Cervix
In view of some of the misunderstanding of the implications of the in situ lesion of the cervix, as well as the strategic role played by the general physician or surgeon in determining how the lesion will be treated, our opinion is presented briefly. Some of the errors in misdiagnosis have already been mentioned earlier in this chapter (p. 155).
Assuming the diagnosis has been carefully arrived at and is correct, it is still important to realize that carcinoma in situ of the cervix may lend itself to relatively conservative management if the all-important trio of clinician, cytopathologist, and patient can be relied upon to work together effectively. The avoidance or postponement of hysterectomy and related procedures is often of real importance since carcinoma in situ occurs fairly frequently in young women of childbearing age and inclination.
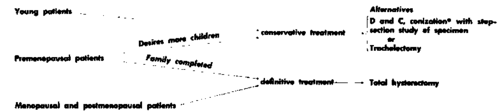
*After conization it is necessary to repeat vaginocervical smears every six months for a minimum of five years.
Fig. 57. Outline of management of carcinoma in situ of the cervix. (From Jordan, M. J., and Bader, G. M.: Early Diagnosis and Management of Cancer of the Female Cenital Tract, CP 21:115-121, I960.).
For the management of in situ carcinoma of the cervix, we endorse the program outlined by Jordan and Bader as shown in Fig. 57.
Continue to:
My Books

