Larynx Cancer
Description
This section is from the book "Cancer Manual For Public Health Nurses", by National Cancer Institute. Also available from Amazon: Cancer Nursing: A Manual For Public Health Nurses.
Larynx Cancer
Cancer of the larynx is treated by both surgery and radiation.
The treatment for early cancer which is confined to certain limited areas of the larynx is usually radiation or a partial-laryn-gectomy (laryngofissure). In this operation the thyroid cartilage is split and a conservative excision of the tumor is performed. The voice box is not removed. The patient may have a temporary tracheostomy to facilitate breathing during the postoperative period. When this is closed the patient is able to speak although he usually has a harsh or hoarse quality to his voice as a result of surgery to the vocal cords.
A total laryngectomy which involves complete removal of the larynx (voice box) is a much more extensive operation. In this procedure the upper portion of the trachea is also removed and the open end of the remaining portion is brought out to the anterior part of the neck and sutured. The opening into this is called the stoma and it is in here the patient wears his laryngectomy tube. As stated elsewhere, some patients eventually get along without a tube, or wear one part of the time. This depends partially on the size of the stoma and its tendency to close down or remain open. All laryngeal structures above the stoma are removed. Thus many of the structures which control the speech mechanism are missing. However, the tongue and many of the soft tissues which play a part in producing speech are left intact. It should also be remembered that the olfactory and taste mechanisms are interfered with, and these patients have difficulty in detecting odors and tasting certain foods.
This is different from a tracheostomy in which all of the structures remain intact and the tube is inserted into the trachea through an opening made through the cartilagenous rings of the trachea. (Figure 9).
Nursing Care
The patient who undergoes a laryngectomy may have a great deal of difficulty accepting loss of speech. However, it is possible for him to learn a special method of speaking called esophageal speech. The nurse may be most anxious to help him learn to communicate. However, it is well to know the physician's plan for the patient's rehabilitation before encouraging the patient to articulate. In the interim she can encourage the patient to use pencil and paper and hand signals to make his wishes known. Many speech therapists, though not all of them, prefer to teach the patients without their having attempted to articulate prior to formal instruction. In some situations the speech therapist will have visited the patient preoperatively and will follow through postoperatively. This is especially helpful if the teacher is himself a person with a laryngectomy. In esophageal speech air which is trapped in the upper esophagus moves upward through the closely approximated membranous surfaces of the cricopharyngeal sphincter into the hypopharynx. The sound is then converted into speech by the lips, tongue, teeth, and palate.5 The quality of the speech varies and is usually harsh and flat in tone. However, with practice, many patients communicate very effectively.
The patient's family should encourage the patient to talk, and should not attempt to anticipate his wants and obviate his need to communicate. This may take a great deal of patience and understanding on the part of everyone concerned.
For those who are unsuccessful at learning to speak or for whom facilities are not available there are several artificial larynx devices on the market. There are many limitations to these but improvements are made from time to time.
The most recent model is a transistor type which resembles a small flashlight or electric shaver. This electronic device is designed to be held against the outside of the throat while it is being operated. It transmits sound waves into the throat, replacing those normally produced by air passing over the vocal cords. Speech is 5 Levin, Nathaniel M., Speech Rehabilitation After Total Removal of Larynx. JAMA, Vol. 149. No. 14. August 2, 1962. p. 1281-1286.
NORMAL AIRWAY
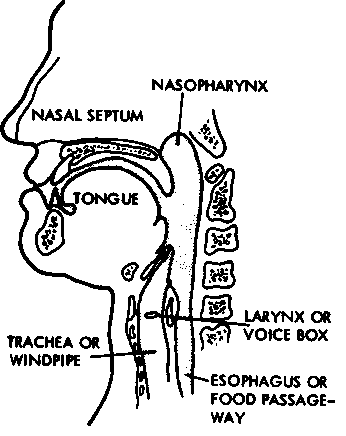
The mouth and neck look this way inside before an operation.
TRACHEOSTOMY

The tracheostomy tube leads right into the windpipe.
LARYNGECTOMY (Removal of the voice box)
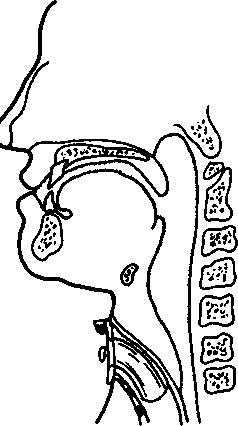
The entire larynx (voice box) is removed. Here a detour is made from the trachea to the skin.
Figure 9 produced by forming words with the teeth, tongue and lips, as in normal talking. The nurse would not recommend this or any other device unless this were part of the physician's plan for rehabilitating the patient. This device is available at cost from the Bell Telephone Co. No profit is made by the manufacturer.
The patient should be cautioned to avoid or modify activities which risk getting water in the stoma. Some patients are able to take showers by angulating the water so that none of it drains into the stoma. Tub baths are possible, too, if the patient is careful and the water in the tub is kept at a low level.
Many patients are able to resume their usual occupation, particularly if their work does not involve much in the way of verbal communication. For those whose work involves talking a great deal, return to work is somewhat dependent upon regaining a method of speech. However, many business men have successfully rehabilitated themselves to the point where they have resumed their former line of work. It is perhaps the contact with the successfully rehabilitated which is the "drawing card" of the laryngectomy clubs which flourish in several cities. Contraindications from an occupational point of view would be laboring jobs which involve contact with dust, steam, or water.
Continue to:
My Books

