Care Of Tracheostomy And Laryngectomy Tubes
Description
This section is from the book "Cancer Manual For Public Health Nurses", by National Cancer Institute. Also available from Amazon: Cancer Nursing: A Manual For Public Health Nurses.
Care Of Tracheostomy And Laryngectomy Tubes
Tracheostomy and laryngectomy tubes look quite similar except that the laryngectomy tube is thicker and shorter. Each comes in several sizes and each has three parts, an outer cannula, an inner cannula, and an obturator. The obturator is used at the time of insertion and must therefore be accessible at all times. Some tubes are made of soft silver and these will dent if dropped. Plastic tubes are now available in some areas. (Figure 10).
Removing Tubes
It is essential that both tracheostomy tubes and laryngectomy tubes remain patent at all times. The inner cannula of either kind may be removed by the nurse for cleaning. The outer cannula is never changed except on the specific order of the physician. A nurse will seldom have occasion to change a tracheostomy tube. This procedure is somewhat hazardous since the tracheostomy tends to close up when the tube is removed and there is some danger that the nurse may not be able to reinsert the tube. Laryngectomy stomas are much larger and do not close as readily. In fact, many patients do not use their tubes at all after a certain length of time.
Cleaning Tubes
Tubes may be cleaned with soap and water, a mixture of hydrogen peroxide and water or one of many other cleaning solvents on the market. Accumulated secretions may be removed with a small brush or strips of gauze may be pulled through with a forceps. Brushes should be replaced frequently since loose bristles may adhere to the tube. After the tube has been cleaned it should be thoroughly rinsed before it is replaced.
A. laryngectomy tube
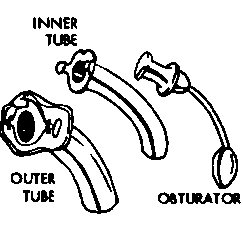
B. tracheostomy tube

Note: The laryngectomy tube is shorter and bigger in circumference.
Figure 10.
Changing Tubes
To change a tube insert the obturator into the outer cannula:
(1) Lubricate the tip lightly with cottonseed or olive oil.
(2) Hold tube between index and middle fingers of right hand. Support obturator with thumb.
(3) Gently, insert the outer cannula into the wound with a downward and inward motion until the shoulders of the cannula rest against the patient's neck.
(4) Immediately remove obturator to prevent coughing and obstruction to breathing.
(5) Tie the tapes gently but securely behind the patient's neck. Do not tie a bow knot as this may slip or become undone.
(6) Insert inner cannula. Lock in place.
(7) Separate cut sections of 4 inches by 4 inches gauze square and slip under shoulders of laryngectomy tube and up until cut ends meet. Do not use cotton-filled gauze as there is danger of the cotton becoming loose and obstructing the airway. (Figure 11).
A. 4 x 4" Gauze Dressing
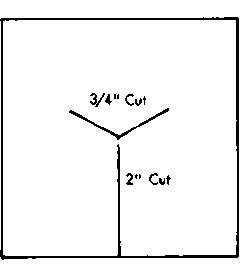
B. Laryngectomy Dressing

Figure 11
Continue to:
My Books

