Oral Cavity Cancer
Description
This section is from the book "Cancer Manual For Public Health Nurses", by National Cancer Institute. Also available from Amazon: Cancer Nursing: A Manual For Public Health Nurses.
Oral Cavity Cancer
Cancer of the oral cavity is a general term which denotes a variety of tumors occurring either outside the mouth on the upper or lower lip, or within the mouth on the tongue, floor of the mouth, buccal mucosa, gingiva, and hard palate. Tumors of the lower jaw are also included in this general term of designation.
As one would expect, treatment for this wide range of tumors varies considerably, and depends upon the location of the lesion, its individual characteristics, the expected clinical course, and the prognosis. In some instances, radiation is the treatment of choice, but other tumors may be treated surgically. Occasionally the same tumor is treated with both radiation and surgery.
In addition to the treatment for his primary lesion the patient is often subjected to additional procedures required to control spread of his cancer. For example, a radical neck dissection, either unilateral or bilateral, is fairly common. This is often accompanied by a temporary tracheostomy since postoperative swelling might otherwise cause respiratory embarrassment.
Nursing Care for Oral Cavity Cancer
Many of these surgical procedures result in speech defects of varying degrees, in scarring, or changes in facial contour. It is therefore sometimes difficult for the patient to accept his altered appearance or speech. The nurse can often be helpful in working with the patient to make it more possible for him to accept himself as he is. The family sometimes needs help, too, in accepting the patient and helping him to regain his self-confidence.
In some instances the speech defect may warrant referral to a speech therapist. Other patients may be able to get along without professional help but may have to devote much personal time and effort to correcting faulty enunciation.
It would be impossible in a manual of this size to quote specific nursing care measures for every tumor of the head and neck region. Certain general nursing procedures commonly employed are as follows:
Packing
Resections of the oral cavity may leave depressions or sinuses. These are usually packed daily with one of several kinds of impregnated gauze. This packing which serves to promote healing and to reduce odor, must be removed at specified intervals. Very often this is followed by a mouth irrigation before new packing is inserted.
Irrigations
Mouth irrigations can be given with either a bulb syringe or by means of the usual irrigating can with rubber tubing. All glass tubes should be rubber tipped to prevent injury to the mouth. Using too much force may cause injury to delicate tissues which are in the process of healing and may also cause gagging. It is therefore important to keep irrigating cans at a low level (approximately one foot above the patient's shoulder) and to avoid hard pressure on the rubber bulb if a bulb syringe is used. The solution will vary: Among the common ones are normal saline, salt and soda, sodium bicarbonate, or hydrogen peroxide and water. Be sure to remind the patient to hold his breath (or exhale) while irrigating; the tubing should be pinched off while the patient takes a breath.
Dressings
It is seldom that the patient will still be using dressings after he has returned home from the hospital. If sterile dressings should be needed someone in the family should be instructed in the technique of how to apply them. In some instances the supply of dressings may pose a problem and the nurse may have to call upon a community resource which will offer them free of charge.
Prosthesis
Many patients who have oral resections are fitted with prosthetic devices to replace missing structures. These vary from small obturators to very extensive and quite complicated jaw-replacement mechanisms. The nurse should find out what directions the physician or dentist has given the patient relative to the care of any special equipment of this nature. She should also encourage the patient to use the device even though it is difficult for him to become accustomed to it. (Figure 12).
Special Feedings
Patients with extensive resections of the oral cavity may have difficulty in eating the usual family diet. Soft, nonirritating foods of the consistency of baby and junior commercial foods are easily swallowed. Food can also be prepared with a food mill, a ricer, or a blender. By using a food blender, almost any food can be reduced to a liquid state. There is comfort to both patient and family in using "regular" foods. Care must be taken that all the essential food elements are included in sufficient amounts. An occasional review of a day's intake will serve to check on the adequacy of the diet. Some patients require tube feedings. See appendix II for suggested feedings.
Tracheostomy Care
A tracheostomy which was done pro-phylatically at the time of surgery will almost always be closed by the time the patient returns home. In rare instances in which subsequent developments prohibit or delay closing the opening the nurse may have to teach some of the important points to be remembered. Be sure the patient understands that this tube constitutes his airway, and that removal might jeopardize his life. For this reason it is well to use a firm knot to tie the tape which holds the tube in place. Bow knots tend to slip open and should not be used. Most patients who have a tracheostomy are able to talk if they cover the tube opening with a finger. (This reestablishes continuity of the airway.) For care and changing of the tube see section on care of laryngectomy and tracheostomy tubes, page 47.
Reconstructive Surgery Of The Face
Much of the surgery for cancer of the face is extremely radical and reconstructive surgery may be undertaken to either improve the appearance of the patient or to increase his ability to function adequately. This is often plastic surgery which involves special grafts, pedicles, skin flaps, etc. This kind of surgery takes great skill and is very time consuming. It is difficult for the patient who undergoes the treatment and he may be handicapped physically, emotionally, and financially for many months.
It is important for the nurse to have specific orders about the care of these patients. Suture areas must be kept clean; immobilization of certain areas may be essential and she should also be quite

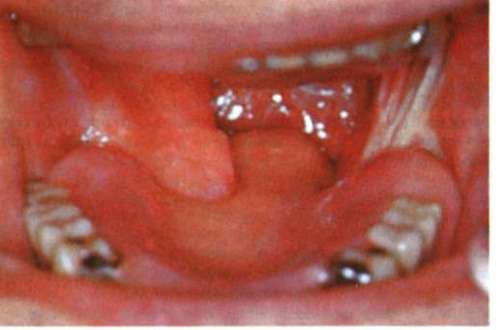
TOP: Oral Resection. BELOW: Prosthesis in place.
Figure 12 alert to the possibility of loss of circulation in special pedicle grafts. The nurse should watch for changes in skin color of the graft, temperature changes, sloughing, or infection. Not the least of her tasks is to help the patient accept the protracted wait which is involved.
Continue to:
My Books

