Female Reproductive Organs
Description
This section is from the book "Cancer Manual For Public Health Nurses", by National Cancer Institute. Also available from Amazon: Cancer Nursing: A Manual For Public Health Nurses.
Female Reproductive Organs
Cancer of the cervix is asymptomatic in the very early or beginning stage when the chance for cure is greatest. It is this cancer which is too early to be detected on inspection which may be discovered by the study of cells removed for cytologic examination. Biopsy is employed to confirm suspicious cytologic findings. The early noninvasive lesion of the cervix is sometimes called carcinoma in situ. Methods of treatment vary markedly and include conization, amputation of the cervix, or hysterectomy. Some physicians temporarily withhold therapy, especially if the woman is in the child-bearing age group, and keep close watch on the status of the lesion and the condition of the patient.
Cancer of the cervix which has become invasive is also treated in a variety of ways, depending upon the stage of the disease, the individual patient, and the judgment of the physician. Surgery sometimes involves removal of the ovaries and Fallopian tubes as well as the uterus itself. Node dissections may be fairly limited, or quite extensive as in a Wertheim operation.
Radiation therapy, either X-ray or radium may also be used in treating carcinoma of the cervix. In some instances both surgery and radiation therapy are employed in treating the same patient. See page 63 for care of patients receiving radiation therapy.
Nursing care for patients who return home after one of the more complicated hysterectomy procedures which involves the removal of pelvic nodes or resection close to the bladder may necessitate some degree of bladder retraining. Function may be temporarily impaired by the surgery.
Cancer of the body of the uterus arises from the endometrial lining. Because this is a vascular area, bleeding tends to occur during the early stages of the disease. Diagnosis is usually made by curettage. Treatment is irradiation, a combination of irradiation and surgery, or surgery alone.
The nursing care of these patients is similar to that which is given to any patient receiving radiation or having major abdominal surgery. Occasionally the bladder or bowel is affected as a result of the treatment and special attention may be required to restore normal function.
Cancer of the vulva ranks third in the frequency of all female genital cancers. It is usually treated by surgery. The surgical procedure tends to be radical, and involves the removal of several very vital structures. Patients who return home after the surgery may still require dressings, perineal care, or sitz baths. They often find it difficult to sit comfortably.
Public health nurses should be alert to the possibility of case finding among older women in the home, or special institutions as nursing homes, and homes for the chronically ill, since most cancer of the vulva occurs in post menopausal women. Patients with complaints relative to pruritus or other discomfort should be referred for medical evaluation.
Cancer of the ovary has an insidious onset and is difficult to diagnose until enlargement or asymmetry of the abdomen is discovered. Surgery is usually the treatment of choice. Radiation therapy and chemotherapy may be used as adjuncts or for palliative purposes. The care following surgery is the same as that given for other types of abdominal surgery.
If ascites develops because of metastatic spread of ovarian cancer the patient may be hospitalized and treated by the intracavitary injection of radioactive gold. This limits the fluid formation and lessens the need for paracentesis. Also, the patient is more comfortable due to diminution in the amount of fluid in the abdomen.
Nursing care for these patients, while they are at home, is largely supportive with attention to diet, fluid intake, and adequate rest. When marked ascites occurs, physical movement of the patient may be difficult. However, ambulation should be encouraged for as long a time as possible.
Cancer in any part of the female reproductive system inevitably poses new problems for the patient. Among these are the creation of an artificial menopause, change in the way the patient perceives herself as a woman, and her concern as to how her husband will accept her.
Surgery for Advanced Pelvic Cancer
In recent years various types of radical surgery have been undertaken in the attempt to better the survival rates for women with advanced pelvic cancer. In fact there are reports in the literature citing survival rates of 5 to 12 years. Occasionally this radical surgery is curative since cervical cancer often remains confined within the pelvis for long periods of time. These operations are done for cancer of the cervix, corpus, vagina, vulva, and sometimes the rectum.
There are three types of surgical procedures which may be performed:
1. Anterior exenteration for cancer which has spread anteriorly to the bladder. The rectum is preserved and the bladder, uterus, adenexa, and vagina are removed. (See diagram A). The ureters are transplanted into an isolated loop of the sigmoid or into a special pouch of the ileum, forming the so-called ileal bladder.
2. Posterior exenteration for cancer which has spread into the rectum. This spares the bladder and removes the uterus, adenexa, and the rectum. (See diagram B). The patient has a colostomy.
3. Total exenteration involves removal of the uterus, adenexa, lymphatic channels, lymph nodes, bladder, rectum, vagina, and vulva. (See diagram C). The patient has a colostomy and the ureters are transplanted into an ileal bladder or isolated loop of the colon. (See diagram D).
These major operative procedures are done only if the surgeon thinks he can remove all of the carcinoma. They are not done if there is bony invasion or distant metastases.
These procedures avoid the "wet colostomy" which involves transplanting the ureters into the colon and allowing the urine, along with the feces to drain through the colostomy opening. Separate openings for urine and feces facilitate the collection of urine and permit caring for the colostomy in the usual manner. (See diagram E).
Nursing Care
If the surgery involves formation of a colostomy (assuming this is not a "wet colostomy") the care involved would be the same as that for any dry colostomy. See page 37.
The ileal bladder is a conduit for urine only. The urine drains through a special opening on the abdominal wall into a collection bag. The ileal bladder is NEVER IRRIGATED.
A wet colostomy is different because both urine and feces drain from the colostomy opening. The collection bag will therefore be somewhat different in size and shape. Wet colostomies are NEVER IRRIGATED since there is danger of an ascending infection via the ureters. As stated heretofore the wet colostomy procedure has been largely replaced by the ileal bladder technique.
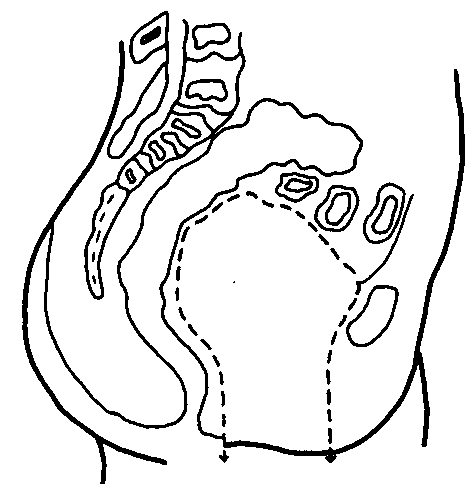
ANTERIOR PELVIC EXENTERATION. Genital Organs and Bladder Removed. Diagram A
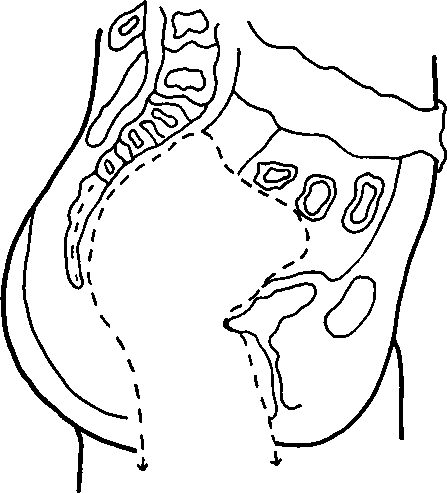
POSTERIOR PELVIC EXENTERATION. Rectum and Genital Organs Removed. Diagram B
COMPLETE PELVIC EXENTERATION. Genital Organs. Bladder and Rectum Removed. Diagram C

Continue to:
My Books

