Inhibition Of Human Mammary And Prostatic Cancers. Part 2
Description
This section is from the book "The Scientific Contributions Of The Ben May Laboratory For Cancer Research", by The University of Chicago. Also available from Amazon: The Scientific Contributions Of The Ben May Laboratory For Cancer Research.
Inhibition Of Human Mammary And Prostatic Cancers. Part 2
Cortisone has made possible this satisfactory replacement regimen. In our experience 25 mg. of cortisone acetate by mouth twice daily and the oral ingestion of 3 gm. of sodium chloride in most cases gave excellent results. Some of our patients have been maintained on as low as 12.5 mg. cortisone acetate twice a day with 3 gm. of salt, while other patients have required 2-4 mg. of DOCA daily in addition to cortisone acetate and salt to prevent orthostatic hypotension. The orthostatic hypotension occasionally seen was not corrected by augmenting the sodium chloride intake or even raising cortisone acetate to above 75 mg. a day. To increase the cortisone acetate above 50 mg. a day does not seem wise, for at these levels the protein catabolic effect becomes too predominant. The majority of the cancer patients after operation have an excellent appetite and gain weight rapidly.
When the patient is on an adequate hormonal maintenance, the glucose tolerance test, insulin tolerance test, and water diuresis test are normal and similar to those in the pre-operative period. In two patients with diabetes mellitus there has been no significant change in the insulin requirement.
When maintained adequately, adrenalectomized patients have a healthy appearance, are not incapacitated, and they are able to engage in all their usual activities. Cutaneous pigmentation of the addisonian type does not occur. Six of the patients, including four males and two females, had hot flushes, but these vasomotor changes disappeared within 3 months. The patients withstand well the common ordeals of life. Under severe emergencies, such as extreme heat and severe infections, signs of adrenal insufficiency develop occasionally, but these were easily eliminated by increasing the amount of cortisone acetate and DOCA.
On our hormonal maintenance schedule the total protein content and least thermocoagulable protein percentage of serum can reach normal values and the erythrocyte number and hemoglobin content of whole blood as well.
Adrenalectomy For Cancer Of The Prostate
In this series of seven patients there was one post-operative death (Case 3), leaving six effective cases of prostatic cancer. Another patient (Case 4) died of acute pulmonary edema 49 days after adrenalectomy.
In four of the patients the primary tumor was large and nodular; the neoplasm decreased appreciably, as determined by palpation in two of these men, while in two other cases it was unaffected. In two cases in this series the prostate was atrophic at the time of adrenalectomy because of previous anti-androgenic control, and the gland underwent no further change; both of these patients were incapacitated because of metastatic lesions.
All the patients gained weight after adrenalectomy. In five patients the hemoglobin concentration (Table 1) increased, and in three patients there was an increase in the total number of erythrocytes. In three patients there was an increase in the total protein concentration (Chart 1), and in four patients there was a decrease of the least coagulable percentage of serum.
A large increase of acid phosphatase in serum was present before adrenalectomy only in two patients; in both cases there was a significant decrease in the level of this enzyme (Chart 2), but the decrease was not so precipitous as usually occurs in a previously untreated case of prostatic cancer after orchiectomy.
Perhaps the most striking observation has been the immediate and persistent relief of crippling pain in the bones. All the six patients in this series suffered from this complaint, and the pain was of such severity that all of them had been treated by morphine or codeine prior to adrenalectomy. In one patient (Case 7) there was no diminution of pain; in five patients the pain was completely relieved within 2 days after adrenalectomy, and the relief has persisted during the observational period. We are of the opinion that three of the six patients (Cases 2, 5, 6) in this series have had a clinical remission of the disease of considerable magnitude.
Adrenalectomy For Mammary Cancer
This procedure was carried out on seven patients in this category. There was one post-operative death (Case 8) leaving six effective cases. One patient (Case 10) died 23 days after adrenalectomy.
Table 1. Whole Blood And Blood Sebum Values After Adrenalectomy In Cancer
Prostatic cancer
Least | Serum phoaphatases | |||||||
Hemoglobin | Erythrocytes | Total protein | coagulable | acid | alkaline | |||
Case | Days | gm/100 ml | X 10^6c. mm | gm/100 ml | (per cent) | units/100 ml | ||
1. E.S. | Pre-operative | 13 | 4.37 | 6.90 | 83 | 4.0 | 11.1 | |
Post-operative | 251 | 12 | 8.88 | 7.47 | 20 | 6.9 | 11.8 | |
2. CF. | Pre-operative | 13.4 | 4.19 | 6.40 | 26 | 18.9 | 26.2 | |
Post-operative | 240 | 17.4 | 5.83 | 7.88 | 20 | 7.0 | 11.1 | |
S. J.S. | Pre-operative | 10.5 | 3.89 | 7.30 | 84 | 4.4 | 12.3 | |
4. L.S. | Pre-operative | 12.2 | 4.84 | 7.09 | 26 | 4.5 | 8.5 | |
Post-operative | 47 | 13.5 | 4.12 | 6.31 | 25 | 8.4 | 4.6 | |
5. W.M. | Pre-operative | 11 | 3.16 | 6.13 | SO | 92.8 | 80.6 | |
Post-operative | 180 | 13 | 4.03 | 7.11 | 20 | 32.3 | 33.9 | |
6. J F. | Pre-operative | 12.2 | 4.02 | 6.28 | 24 | 4.0 | 6.8 | |
Post-operative | 158 | 13.3 | 4.12 | 7.13 | 18 | 3.0 | 7.0 | |
7. G.H. | Pre-operative | 8.0 | 3.26 | 6.92 | 32 | 4.3 | 28.5 | |
Post-operative | 187 | 9.5 | 2.87 | 5.59 | 41 | 2.0 | 18.8 | |
Mammary cancer | ||||||||
8. L.C. | Pre-operative | 12.8 | 3.91 | 5.23 | 27 | 6.7 | 6.0 | |
9. MB. | Pre-operative | 13 | 3.99 | 7.08 | 23 | 4.2 | 10.7 | |
Post-operative | 168 | 13.5 | 4.13 | 5.99 | 24 | 6.4 | 12.6 | |
10. R.B. | Pre-operative | 11.5 | 4.0 | 6.22 | 28 | 0.8 | 7.2 | |
Post-operative | 19 | 13.0 | 4 4 | 6.12 | S8 | 2.6 | 6.3 | |
11. J.B. | Pre-operative | 10.6 | 3.47 | 5.77 | 29 | 4.4 | 5.6 | |
Post-operative | 156 | 12.0 | 4.08 | 5.91 | 30 | 1.7 | 9.6 | |
12. G.N. | Pre-operative | 12.0 | 4.41 | 6.21 | 26 | 4.6 | 9.9 | |
Post-operative | 155 | 11.5 | 3.80 | 6.88 | 22 | 6.0 | 8.1 | |
13. N.C. | Pre-operative | 15 | 5.04 | 6.00 | 22 | 3.4 | 4.6 | |
Post-operative | 117 | 18.4 | 4.01 | 6.65 | 20 | 4.2 | 6.0 | |
Among the six effective cases, the course of the disease was not influenced favorably in two patients (Cases 10,11); in one case there was minor improvement (Case 9); some regression of the lesions was observed in three cases (Cases 12, 13, 14).
In Case 10 there were extensive pulmonary metastases, and the patient suffered from dyspnea; the lesions seemed to be completely unaffected by adrenalectomy. In Case 11, there were large sloughing ulcerations of cancers of each breast; following adrenalectomy the ulcerative process advanced rapidly.
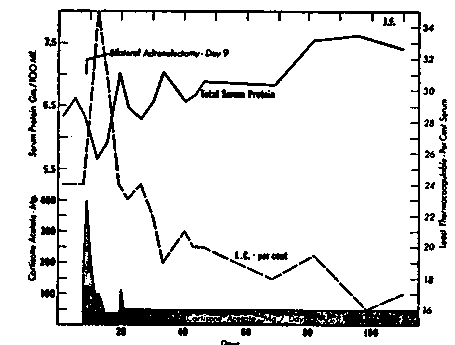
Chart 1.-Increase of total protein and decrease of least percentage of thermocoagulable protein of serum in a patient (Case 8) with metastatic cancer of the prostate. L.C.-Least thermocoagulable protein of serum.
One patient (Case 9) was moderately improved in that pain decreased and body weight increased after adrenalectomy and excision of the ovaries. The osseous metastases in this person had been advancing rapidly prior to adrenalectomy. Following removal of gonads and adrenals the advance seems to have been retarded, and there has been slight and partial recalcification of the lesions.
In two patients (Cases 12, 13), both with pulmonary metastases, there has been an increase in the total serum proteins together with a decrease in least coagulable percentage of serum and regression of pulmonary metastases as determined by radiography. In a man (Case 13) with evidence of intracranial metastases and large pulmonary metastases as well, there was a significant decrease (Figs. 1, 2) of both lesions within 8 weeks after adrenalectomy, and the gains are still maintained after 4 months.
In one woman (Case 14) there was a decrease (Figs. 3, 4) in the size of cutaneous metastases of mammary cancer in a post-mastectomy scar noted within 2 weeks after adrenalectomy and in a large tumor of the contralateral breast also. The regression was accompanied by evidence of involution as determined by cytologic methods on biopsy specimens (Figs. 5, 6).
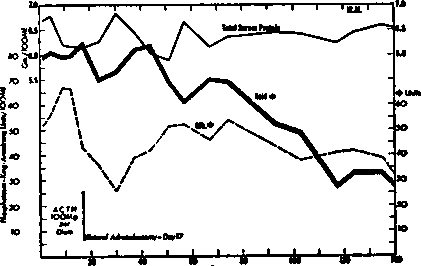
Chart 2.-Decrease of level of acid phosphatase of serum after adrenalectomy in a patient (Case 5) with metastatic cancer of the prostate.
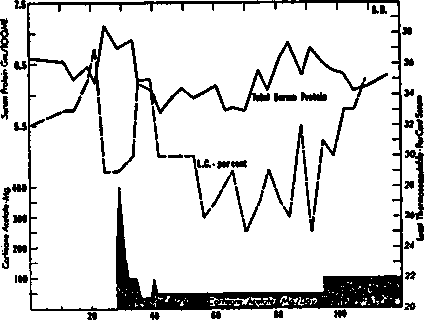
Chart 3.-Decrease of total protein and increase of least percentage of thermocoagulable protein of serum at cortisone acetate levels above 50 mg. daily in a patient with prostatic cancer.
Adrenalectomy for miscellaneous tumors.-There were four patients in this series with advanced cancer (squamous carcinoma, melanosarcoma, chorionic epithelioma, and an undifferentiated carcinoma) other than that of the breast and prostate. All had extensive metastases. They have been followed for 1-3 months after adrenalectomy. Adrenalectomy had no detectable effect in retarding the growth of these tumors. To the contrary, positive evidence was obtained of increase in size of the cancers in all of them.
Treatment of prostatic cancer by cortisone acetate and ACTH.-Pituitary adrenocorticotrophin (ACTH), 100 mg. daily for 14 days, was administered to three patients with advanced cancer of the prostate with metastases. Cortisone acetate was injected intramuscularly in four similar cases for periods up to 90 days, the dosage being exactly that used in the medical management of the patients subjected to bilateral adrenalectomy.
Continue to:
My Books

