Chapter XXVIII. Diseases Of The Spinal Cord
Description
This section is from the book "A Manual Of Pathology", by Guthrie McConnell. Also available from Amazon: A Manual Of Pathology.
Chapter XXVIII. Diseases Of The Spinal Cord
Circulatory Disturbances
Anemia of the cord may be due to pressure from neoplasms or to obstruction of small blood-vessels by disease or thrombosis. Embolism is followed by necrosis. In pernicious anemia degenerative changes in the posterior columns of the cord may occur.
Hyperemia is present in all inflammations of the meninges or cord. Passive hyperemia is present in chronic heart and lung disease. Antemortem congestion is difficult to differentiate, as there is nearly always hypostasis of the blood into the spinal vessels.
Hemorrhage into the cord is less common than in the brain. It may be punctate or massive. The punctate form occurs in death from convulsions, as in tetanus, after injuries, in degenerated areas, about tumors, after extreme congestion, and in other conditions. Massive hemorrhages are seldom larger than a small marble. They may find a way along the longitudinal fibers or occasionally rupture into the central canal.
The changes that take place if the individual lives are similar to those occurring in the brain under like conditions.
Myelitis, although strictly signifying an inflammation of the spinal substance, is used to indicate any form of degeneration present in the cord. It may be primary or secondary. The primary form occurs at the seat of the injury, and is frequently a circumscribed condition. Secondary degeneration depends upon primary changes elsewhere, and is due to the destruction of nerve-cells or axis-cylinders. It is generally considerably more extensive than a primary degeneration. The degenerated areas may be white, red, or yellow, according to the amount of blood present and the stage of the softening. In the early stages the involved tissue is swollen and pinkish, and minute hemorrhages may be present. The tissue is at first softened, but finally becomes firmer as fibrous changes occur. Microscopically the myelin is found to be destroyed, breaking down into droplets that stain with osmic acid. The axis-cylinders swell up and degenerate, the nerve-cells show enlargement and finally disappearance of their nuclei. The tissues generally become disorganized and give rise to white softening, there being no change in color. If the damage to the cord has been such as to cause extravasation of blood into the involved area, it will be known as red softening. As the blood is destroyed the pigment is set free, with the formation of areas of yellow softening.
In purulent myelitis there will be found a round-cell infiltration in the perivascular spaces, pus in the pia mater, and degeneration of the neighboring nerve-tissues. The ganglion-cells, though very resistant, sooner or later show degenerations.
When the acute processes subside, there is some absorption of the broken-down tissues and a hyperplasia of the neuroglia and connective tissue, constituting the early stage of sclerosis. The newly formed tissue is grayish in color, firm, dense, and dry. There is probably little, if any, attempt toward the regeneration of the nerve-fibers.
Myelitis may be traumatic, infectious, toxic, or nutritional.
Traumatic myelitis may result rapidly, but it is usually slow, as a result of compression of the cord by tumors or collections of fluid in the spinal canal. The degeneration generally extends entirely across the cord, being known as transverse myelitis. There are usually three stages, that of red softening, of yellow softening, and of gray degeneration, and connective-tissue hyperplasia.
Infectious myelitis may be transverse or disseminated, particularly the latter. Micro-organisms are generally present in the lesions.
Varieties Of Myelitis
When the spinal membranes are inflamed, the condition is known as spinal meningitis; if the membranes and cord are both affected, meningomyelitis.
Inflammation of the cord alone is known as myelitis; disease of the white substance is leukomyelitis; if the gray matter, poliomyelitis.
Myelitis is referred to as central when arising from disease of the central canal; diffuse, if it involves the entire cord; transverse, when a small section is entirely affected; disseminated, when there are numerous small areas more or less widely separated.
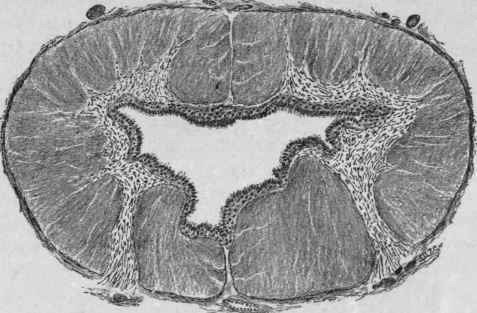
Fig. 184. - Hydromyelia (Partly Diagrammatic) (Stengel).
It may be simple, hemorrhagic, or purulent, or, according to development, acute or chronic.
Hydromyelia is a condition in which the central canal of the spinal cord is dilated by an increased amount of cerebrospinal fluid. The dilatation may be irregular, usually being more marked in the lumbar cord. The canal may be round, slit-like, or triangular, and is commonly lined by ependymal cells, a condition that does not exist normally. Sometimes the canal may be double or even triple, this being more frequent in the lumbar region. Hematomyelia refers to the presence of blood in the central canal; pyomyelia, when pus is present.
Syringomyelia is characterized by a central dilatation of the spinal canal resulting from the proliferation of the glia about the central canal and subsequent degeneration of the newly found tissue.
The appearance is somewhat similar to that in hydro-myelia, but the canal is not lined by ependymal cells.
The etiology of the condition is unknown. There is an extensive proliferation of gliar tissue around the central canal, probably beginning in the cervical portion, but extending down the cord. This tissue rapidly degenerates and liquefies. The cavity is generally posterior to the center of the cord, and may be so large as to leave merely a thin layer of nerve tissue surrounding it. The canal in the early stages is filled with a brownish, gelatinous mass, which eventually undergoes liquefaction, leaving the canal filled with clear fluid.
The extent of the secondary degeneration in the spinal cord and in the anterior and posterior nerve-roots will depend upon the size of the lesion and the amount of pressure exerted. Entire columns of the cord and anterior and posterior nerve-roots may be destroyed in severe cases.
Tuberculosis of the cord commonly involves the meninges, and secondarily extends into the nervous tissues; it is a meningomyelitis. Tubercles are present in varying numbers, and soon cause thickenings and necrosis. Disseminated tubercles may be seen in both the white and the gray matter, but are usually microscopic. Primary tuberculosis may occur in the form of a single circumscribed caseous mass.
Syphilis of the cord usually appears as a thickening of the membranes, especially of the dura. Involvement of the pia and arachnoid is uncommon. There is found a marked endarteritis, and the formation of thrombi is quite frequent. Areas of cheesy degeneration are due to the breaking-down of the diseased tissue.
Tumors Of The Cord
The most common form is the glioma, as occurring in syringomyelia. It infiltrates the nerve tissue along the posterior portion of the cord. It seldom occurs as a circumscribed growth. Sarcoma, cylindroma, and fibroma are very rare, but have been observed.
Tumors of the spinal meninges are more common. Practically all varieties have been found.
Cysts are extremely rare, but both the echinococcus and the cysticercus have been reported.
Continue to:
My Books

