Metamorphoses Of Thrombi
Description
This section is from the book "A Manual Of Pathology", by Guthrie McConnell. Also available from Amazon: A Manual Of Pathology.
Metamorphoses Of Thrombi
The ultimate fate of thrombi depends upon whether they are septic or aseptic. If septic, they must undergo disintegration. If aseptic, they may 4 undergo organization - a condition that is not a transformation into, but is a replacement by, connective tissue.
They may undergo a central liquefaction or softening. The interior is broken down, blood-pigment set free, and leukocytes in varying numbers are present.
Calcification, particularly of small thrombi, giving rise to either arterioliths or phleboliths, according to whether they occur in arteries or in veins.
The connective tissue that replaces the thrombi will gradually undergo contraction until only a hard fibrous mass remains, the original lesion becoming converted into a scar.
The new tissue is derived from the endothelium of the bloodvessel and the fixed connective-tissue cells. As it forms, the thrombus undergoes absorption and breaks down into a mass, the granules of which are removed by the leukocytes.
If the thrombi contain living organisms they will be carried through the circulation and give rise to metastatic abscesses in various parts of the body.
The broken-down portions may become lodged in small vessels, and, acting as emboli, give rise to the condition known as embolism.
Embolism is the obstruction, complete or incomplete, of a blood-vessel due to the lodgment of a foreign body within that vessel, the circulating body being known as an embolus.
The most common variety of embolus is a dislodged portion of a thrombus, particularly those that occur upon the valves of the heart. Other emboli may be formed by cells of malignant tumors, masses of bacteria, blood parasites, particles of fat, pigment, air, etc.
The most common locality for emboli is within branches of the pulmonary artery, with immediate death or respiratory embarrassment resulting. The condition is most serious when vessels supplying important organs, as the brain, spleen, kidney, etc., are obstructed.
The varieties of emboli are: (I) Simple, mechanical, or aseptic; (2) specific, infectious, or septic.
The latter is the more severe, as in it suppurative conditions are associated with the mechanical.
Retrograde embolism occurs when, as in whooping-cough, the intrathoracic pressure is increased. An embolus in the inferior vena cava may be carried in a direction opposite to the blood-current and be thus conveyed into the liver through the hepatic vein.
Crossed or paradoxic embolism occurs when the foramen ovale remains patulous. In this condition an embolus may pass directly from the venous to the general circulation without going through the pulmonary vessels. The results of embolism are numerous:
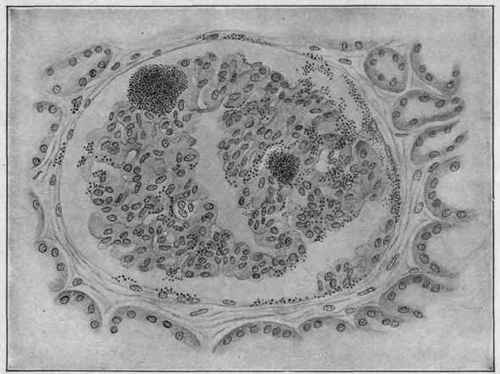
Fig. 4. - Infectious Embolism of the Kidney Following Endocarditis and Showing Groups of Staphylococci in a Glomerulus (Dürck).
1. Thrombosis is a consequence of the stoppage of the flow of blood by the foreign body. The resulting thrombus may be much more extensive than the primary embolus.
2. Inflammation of the vessel walls is usually the result of the lodgment of the embolus, particularly if it is of the infectious type.
3. Atrophy may follow if the blood-supply is not quite enough for the normal demands, but is yet sufficient to prevent actual death of the tissues.
4. Necrosis when the nutrition of a comparatively small area is cut off. Occurs chiefly in the internal organs.
5. Gangrene may result if the main artery of a part has been obstructed and the collateral circulation has been insufficient or unable to supply the demands.
6. Aneurysmal dilatation, especially in the brain, sometimes results.
7. Infarction.
Continue to:
My Books

