X-Ray Technique
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
X-Ray Technique
Gastric cytologic study involves the collection of aspirated material from the stomach and its concentration, staining, and screening for malignant cells. To increase the number of cells available for microscopic study, a number of techniques have been designed to promote exfoliation of cells from the gastric mucosa. These may be divided into two categories:
1. Mechanical. An abrasive brush or balloon is introduced into the stomach, and the mucosa is literally scraped to produce a more abundant cell yield.
2. Enzymatic. An enzyme (e.g., papain, chymotrypsin, etc.) is introduced into the stomach. This dissolves the mucin coating the gastric mucosa and releases the cells held in its grip into the lumen whence they can be collected by lavage.
Combinations of the two methods may be used, and there is evidence that saline washing alone may be satisfactory. Essential to success, whatever method is used, are icing and prompt fixation of the specimen. The technique of chymotrypsin lavage will be described here. It should be emphasized that the procurement and handling of the material is of extreme importance. It should be entrusted only to technicians familiar with the details of proper procedure.
Preparatory Instructions To Patient And Physician
1. No upper gastrointestinal x-ray films should be taken for three days prior to examination since barium contamination of cells renders the test inaccurate.
2. Instruct patient not to eat after the evening meal prior to examination. Water is permissible at any time, however, and dehydration should be avoided.
3. If the patient is showing symptoms or signs of pyloric obstruction, he should be hospitalized for this procedure with overnight continuous gastric suction prior to performance of the test.
4. If intubation gastric analysis is also indicated (see p. 182), it should be done at the same time to avoid intubating the patient twice.
5. If indicated:
(a) Administer subcutaneously 50 mg. of Seconal and 0.4 mg. of atropine fifteen minutes prior to examination or
(b) Have the patient gargle fifteen minutes prior to examination with 100 ml. of 1% local anesthetic solution with Benadryl or Pyriben-zamine.
Technique Of Examination
1. Pass a Levin tube through the nose or mouth to the 70 cm. mark. No lubricants except glycerin should be used.
2. Gastric evacuation. Aspirate all material in the stomach. If food particles are present, discontinue the test.
3. Preparatory lavage. Using 100 ml. of Ringer's solution, wash the stomach, repeating until the return is clear.
4. Chymotrypsin lavage:
(a) Add 7 mg. of chymotrypsin to 500 ml. of 0.1 molar acetate buffer at pH 5.6*. Instill through a Levin tube.
(b) Instruct the patient to lie supine and gradually to rotate from the supine position to the right side to a prone position to the left side and back to the supine position for ten minutes. While the patient is rotating, chymotrypsin and buffer solution should be continuously aspirated into the syringe and reinstilled (Fig. 63, A). This activates the solution in the stomach and results in a better specimen.
*Chymotrypsin is available from Armour laboratories in 7 mg. capsules; 0.1 molar acetate buffer is prepared by adding 13.6 Cm. of sodium acetate and 0.6 ml. of glacial acetic acid to 1000 ml. of distilled water. The buffer may be kept for one month in a well-capped brown bottle.
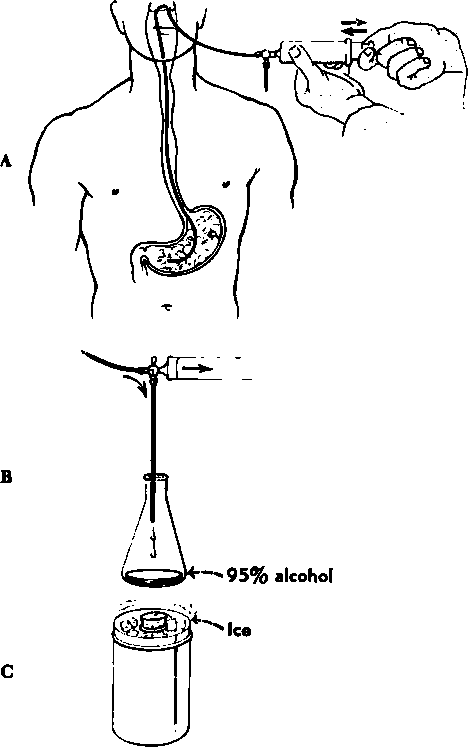
Through a Levin tube introduced nasally or orally, instill, aspirate, and ralnitlll 500 ml. chymotrypsin solution while tho patient is rotating slowly In tho horizontal position.
At the and of 10 minutes, with patient la the left lateral decubitus position, aspirate as quickly and completely as possible into a graduated 1000 ml. bottle. Add an equal volume of 95% ethyl alcohol.
Immediately pack the bottle in ice and deliver to tho laboratory.
Fig. 63. Technique of chymotrypsin lavage.
(c) At the end of ten minutes, while the patient is in the left lateral decubitus position, aspirate as quickly and completely as possible into a graduated 1000 ml. bottle. When aspiration is completed, add an equal volume of 95% alcohol (Fig. 63, B and C). This bottle should be packed in an ice bath and delivered immediately to the laboratory.
(d) In the laboratory the bottle is removed from the ice bath and the contents placed in 50 ml. centrifuge tubes and centrifuged promptly for one half hour at 1500 rpm.
(e) Pour off the supernatant liquid and prepare the smears from the sediment. Use four albuminized slides (two with paper clips). With a clean glass slide, spread the material evenly over the slides so that the final preparation is no thicker than a blood smear.
(f) Alternate clipped slide with undipped slide and place immediately while wet in fixative solution composed of equal parts of ether and 95% alcohol. The paper clips will serve to keep the slides separated.
(g) The slides are now ready for appropriate staining and study.
Findings
The stained specimens must be examined by an experienced cytopathologist. The criteria upon which the diagnosis rests and the microscopic findings encountered will not be dealt with here. A few comments will be made on the reports which may be rendered by the cytologist. The findings are ordinarily classified as positive, suspicious, or negative.
1. A positive report usually indicates the presence of adenocarcinoma cells, and some opinion as to the degree of differentiation may be expressed. Occasionally the diagnosis of malignant lymphoma of the stomach may be made on the basis of gastric cytology. A positive report rendered by an experienced cytologist should be taken as seriously as a positive biopsy.
2. A suspicious report makes repeated gastric cytology studies mandatory. After repeat washings the cytologist can usually render a definite negative or positive report.
3. A negative report by no means rules out the diagnosis of cancer, but if the study was thought to be a satisfactory one, it lessens the chances considerably.
4. Other findings. The study of cells exfoliated from the gastric mucosa has contributed a great deal to an understanding of the wide range of "normal," as well as the findings to be encountered in certain pathologic states, and especially the significance of certain "atypical" cells. The dynamics of gastric physiology and morphology have taken on a new dimension as a result of cytologic studies. Reports have appeared that describe the cytologic findings in cases of atrophic and hypertrophic gastritis, pernicious anemia (treated and untreated), gastric polyps, benign gastric ulcer, the healing phase of gastric and duodenal ulcers, as well as the gastric mucosa following x-ray therapy.
Accuracy
Assuming an experienced cytologist and a satisfactory examination, the over-all accuracy of the method in good hands ranges from 80 to 95%.
1. When the cytologic diagnosis is positive, there is less than one chance in several hundred that the patient does not have cancer (i.e., the incidence of false positives is well under 1%).
2. When the cytologic diagnosis is negative, there is still about one chance in five or six that the patient has cancer (the incidence of false negatives may run from 15 to 20%). The important thing to remember is that when x-ray studies and cytology are both done, the number of cases of stomach cancer undiagnosed or misdiagnosed can be reduced to a minimum. This is due to the fact that the two techniques supplement each other; i.e., a case which is benign or indeterminate on x-ray examination may be positive cytologically and vice versa. Any case which either the cytologist or the radiologist is willing to call cancer should be treated as such. No absolute insistence should be made on agreement between the two techniques.
Continue to:
My Books

