Caffeine. Part 3
Description
This section is from the book "Materia Medica: Pharmacology: Therapeutics Prescription Writing For Students and Practitioners", by Walter A. Bastedo. Also available from Amazon: Materia Medica: Pharmacology: Therapeutics: Prescription Writing for Students and Practitioners.
Caffeine. Part 3
Caffeine as a circulatory stimulant is, therefore, purely an emergency drug, and not one to be used repeatedly. It can in no sense do the work of digitalis. We are inclined to think that much of its apparent value in conditions of low blood-pressure is due, not to circulatory stimulation, but to stimulation of the central nervous system, the brain, cord, and respiratory center, the improvement in muscular tone and respiratory and mental vigor being important in conditions of general weakness.
Respiratory System
Caffeine is a stimulant of the respiratory center, the inspirations being increased in both depth and frequency. In the laboratory this stimulation is best seen after the center has been depressed by narcotic drugs, such as morphine. From 5-grain (0.3 gm.) doses subcutaneously in a man Edsall and Means obtained an increase of the respirations, the oxygen inhaled, the Co2 given off and the alveolar ventilation, without effect on the pulse or blood-pressure. Toxic doses may induce oppressive breathing from excessive action of the respiratory muscles, and eventually exhaust the center, causing asphyxia and death.
Metabolism is increased by large doses, with a slight rise in temperature. From ordinary amounts of coffee or tea there is no essential effect. From 8 to 10 grains (0.5-0.7 gm.) in a man, Means, Aub and Dubois, 1917, find a distinct increase in the basal metabolism with no significant change in pulse-rate, respiratory quotient, proportions of the various food-stuffs metabolized, and the percentage of heat lost through evaporation. Benedict obtained a distinct retention of nitrogen, and "fears that caffeine is not altogether innocuous."
Excretion is fairly rapid. Caffeine tends to lose its methyl groups as it passes through the body, with the formation of dimethyl and monomethyl xanthines, xanthine, and urea; and these, with perhaps some unchanged caffeine, are excreted in the urine. According to most investigators there is no increase in the excretion of uric acid in health; but Schittenhelm (1910) says it is increased, and S. R. Benedict (1916) and Mendel and Wardell (1917) find a definite increase proportioned to the amount of caffeine ingested. In chronic gout Hess and Schmoll, and also Strauss, have determined that both caffeine and theobromine increase the uric acid. In Strauss's case with gout in fingers and knees, a diet of 2 liters of milk, 300 gm. of bread, and 40 gm. of butter gave an average uric-acid excretion of 0.363 gm. per day. On the addition of 2 gm. caffeine (a very large amount) to the day's dietary the uric acid rose to 0.621 gm.
Kidneys
Caffeine is a drug frequently employed in the physiologic investigation of the kidneys, and these investigations have at the same time enlarged our knowledge of the pharmacology of caffeine. It is strongly diuretic, producing diuresis in the isolated kidney just as well as in the intact animal, and in the latter whether general blood-pressure is raised or not; its diuresis is therefore not due to changes in the general circulation. Moreover, local dilatation of the arterioles is not the essential factor, though usually, as measured in an oncometer, the kidney is enlarged during the diuresis and the arterioles are dilated. For diuresis goes on even if the kidney is incased in a plaster cast so that it cannot expand; and there are cases in which, even when it dilates the arterioles, caffeine produces no diuresis. Richards and Plant, in perfusion of the kidney under conditions in which the blood flow was kept constant and independent of the action of the drug, observed diuresis.
To compare urine with the blood from which it is derived, a solution of the dialyzable substances of the blood in the proportions in which they occur in the blood is filtered through an animal membrane, and the filtrate diluted with distilled water until it has the same content of urea as the urine. In this fluid it is found that the proportion of sulphate and phosphate is somewhat more than in the urine, and the proportion of sodium chloride is considerably more (Loewi). This points to a difference in the degree of reabsorption of the different salts by the kidney tubules, the chloride being reabsorbed readily, the sulphate and phosphate with more difficulty, and the urea with the greatest difficulty of all. In caffeine diuresis Loewi finds that the more active it is, the more nearly does the proportion of chlorides to urea in the urine approach their proportion in the blood, a condition that might be expected if the glomerular fluid fails to be subjected to the normal resorption as it passes through the tubules. It would seem, then, that caffeine may perform part of its action as a diuretic by lessening the reabsorptive power of the tubule cells, though it may be that reabsorption fails to take place merely as the result of the increased secretory activity of the tubule cells.
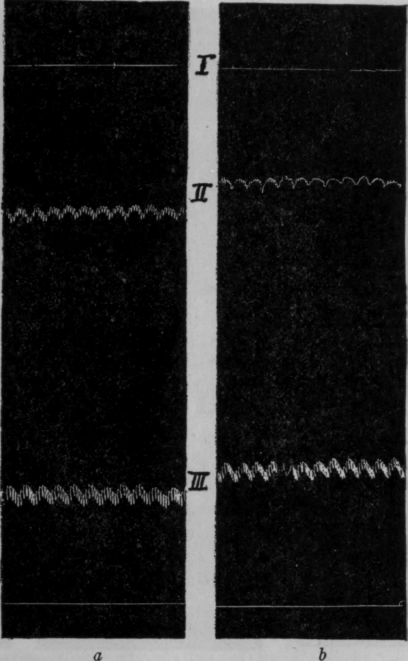
Fig. 34. - Normal dog: I, Drops of urine. II, Kidney volume. III, General arterial pressure: a, Before caffeine; b, fourteen minutes after caffeine (from Pearce, Hill, and Eisenbrey).
Pearce, in his studies of experimental acute nephritis, found that in tubular nephritis caffeine may cause dilatation of the renal vessels, so that the kidney volume is increased as much as in a normal kidney, yet without producing diuresis. And in one of his experimental animals caffeine caused abundant diuresis without producing any increase in the volume of the kidney, i. e., without dilatation of the vessels. In uranium nephritis there was a stage in which caffeine, sodium chloride, sodium sulphate, urea, and dextrose all produced vascular dilatation, yet caffeine was the only one that produced diuresis. His inference was that the diuresis resulted from stimulation of the tubule cells, which are not affected by the other substances.
Continue to:
My Books

