Leg Movements. Part 3
Description
This section is from the book "Massage And Medical Gymnastics", by Emil A. G. Kleen. Also available from Amazon: Massage and medical gymnastics.
Leg Movements. Part 3
Lying Half-Lying Str
grasp-lying Str. -grasp-standing Str.-hanging (2) double Knee-updrawing and -down-pressing.
Lying Knee-Updrawing And-Downpressing
The gymnast stands at the side of the patient and lays one hand as support on his shoulder, while the other is placed upon his knee to give resistance to the exercise.
The patient draws up the knee, resisted by the gymnast, who, when the patient has taken it as far as he can, presses it up passively towards the shoulder as far as possible, after which he presses it back to the starting position while the patient resists.
Repeated three to five times. May be given double by two gymnasts.
Half-Lying Or Stretch-Grasp-Lying Knee-Updrawing And -Downpressing
Like the preceding.
Stretcii-grasp-standing Knee-updrawing and -downpressing (Fig. 60). - Best taken at the wall-bars. Given almost like the preceding, but support is given in the lumbar region instead of at the shoulder.
Stretch-Hanging 2 (Double) Knee-Updrawing And -Down-Pressing
Like the preceding, but double. May be given by one gymnast.
The working muscles are: -
Flexors of hip joint (concentrically and eccentrically); abdominal muscles (statically to fix origin of flexors of hip).
If the movement is done double it also takes place in the joints of the lumbar spine, and the abdominal muscles work concentrically and eccentrically.
Effects And Uses
(a) Strongly repleting to the abdominal and especially to the pelvic organs (according to Brandt). (b) Aids peristalsis.
(c) Impedes respiration; is therefore avoided for weak patients.
(d) Taken double it counteracts lordosis, because the abdominal muscles then contract as much as possible.
Effects Of The Various Starting Positions
Lying and Half-lying positions make the effect of the movement as pure as possible. The latter makes the exercise slightly more difficult, because the origin and insertion of the flexors of the hip are rather nearer together at the beginning of the movement.
Stretch-grasp-lying and Stretch-grasp-standing involve work for many arm and shoulder muscles (statically), so that the movement becomes more complicated, but at the same time easier, because the origin of the working muscles is fixed.
Stretch-hanging is still more difficult and further impedes respiration.
Lying Stretch-lying Leg-lifting and -downpressing.
The gymnast stands at the side of the patient and resists at the feet. The patient raises the leg against the resistance of the gymnast, who then presses it down to the starting position against the resistance of the patient. Can be given double.
(N.B. - If the movement is given for lordosis, the patient should carry the legs up as far as possible, so that the abdominal muscles perform their maximal contraction.)
Leg-raising is practically similar to Knee-updrawing, but is distinguished from it because the leg or legs are kept straight, so that Quadriceps Femoris also works (statically). The movement becomes still harder because the centre of gravity of the legs is brought further away from the hip joint, and because the gymnast's leverage becomes longer. The resistance should be very slight.
High-ride-sitting Backward-falling, Sit-lying Raising, and High-ride-sitting Backward-drawing all take place in the hip joint, and give work chiefly for the same muscles as the other movements of this group, though with the attachments reversed, but they are classified as trunk movements, and described as such, because the trunk is the part moved (see Movements for Abdominal Muscles).

Fig. 60.
B. Combined Flexion in Hip and Knee Joints.
Half-lying Stretch-grasp-lying Short-sitting Leg-updrawing and -downdrawing.
Half-Lying Leg-Updrawing And -Downdrawing
The gymnast stands in front of the patient and grasps with one hand the patient's foot (sole or heel); the other is laid upon the knee. The patient draws up the leg against the resistance of the gymnast, who then draws it back to the starting position against the resistance of the patient. Can also be given as 2 (double) Leg-updrawing and -down-drawing. The gymnast grasps the patient's ankles just above the malleoli.
Stretch - grasp - lying and Short-sitting 2 Leg-updrawing And -Down-Drawing (Fig. 61) are always given double. Short-sitting is taken by the patient sitting on the very edge of a high plinth. An assistant sits in Ride-sitting position behind and fixes him by grasping his shoulders from below.
The working muscles are :
(a) The same as in Knee-updrawing and -downpressing.
(b) Flexors of the knee (concentrically and eccentrically). Effects and Uses. - (a) Similar to Knee-updrawing and down-pressing, but the effect is rather stronger because more muscles work.
(b) Because so many muscles are brought into action at the same time the movement becomes a good one for co-ordination, especially done double, and is used therefore in treating chorea and other diseases where there is disturbance or uncertainty of co-ordination.
Effects Of The Starting Positions
Half-lying and Stretch-grasp-lying have the same effect as in Knee-updrawing.
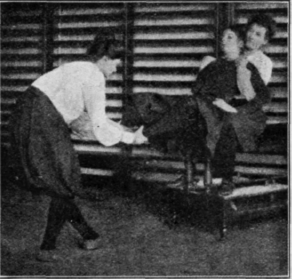
Fig. 61.
Short-sitting is most difficult. It is used especially when the movement is given for lordosis.
C. Movements chiefly for Extensors of Hip.
Back-lean-standing Leg-forward-drawing and -backward-carrying (Fig. 02). - The patient stands with back supported against a wall, usually on a stool. The gymnast stands in front of him and fixes the pelvis with one hand over the Ant. Sup. Iliac spine; with the other hand he grips the patient's leg just above the ankle joint, and so draws the leg forward against the resistance of the patient, who then carries it back to the starting position against the resistance of the gymnast. Repeated four to six times. Can also be taken in Lying position. (N.B. - The supporting leg must not be bent at the knee during the movement.)
The working muscles are : - Extensors of hip (eccentrically and concentrically).
Effects And Uses
Depleting from the pelvis (according to Brandt). To this group belong really also High-ride-sitting Backward-bending and Back-raisings, but because in these movements the trunk is the part moved they are described with trunk movements (see Movements for Extensors of Trunk).
Continue to:
My Books

