Tuberculosis. Part 3. Character Of The Lesion
Description
This section is from the book "A Manual Of Pathology", by Joseph Coats, Lewis K. Sutherland. Also available from Amazon: A Manual Of Pathology.
Tuberculosis. Part 3. Character Of The Lesion
The typical lesion in tuberculosis is the so-called miliary tubercle, and it is this which was referred to above as being the specific product of the action of the virus.
The miliary tubercle is a minute rounded body (Fig. 128) composed of cells and devoid of blood-vessels. A single tubercle is scarcely visible to the naked eye, but, by the confluence of several, there may be larger nodules formed, and even, by the concurrence of vast numbers in successive generations, large masses. At first sight the tubercle seems composed simply of round cells, but closer inspection shows usually three forms to be present. The most peculiar and* typical is the Giant-cell, which in the early stages is nearly a constant constituent. It is a large body (seen in the middle in Fig. 128) presenting at its margin radiating processes, especially at its poles, and containing numerous oval nuclei, usually arranged in a row near the periphery of the cell. The giant-cell is generally near the centre of the tubercle, but may be considerably removed from this position. There are frequently several in one tubercle. The second constituents, the Epithelioid cells, are smaller than the giant-cells and possess one nucleus, but are still of considerable size. They are like the similar cells in the inflammatory new-formation. They surround the giant-cell, and in their general appearance somewhat resemble it. Ordinary round cells or leucocytes form the third constituents, and they are variously abundant according to circumstances. They belong chiefly to the polymorphonuclear variety of leucocytes, and the nuclei stain deeply. They are present at first at the periphery, and may be regarded as representing the ordinary inflammatory products, which are commonly seen in the tissue around. The giant-cells and epithelioid cells seem to be the essential constituents of tubercles, and in perfectly recent examples they may be almost the only ones. They are, according to Baumgarten, the immediate products of the action of the tubercle bacilli, the leucocytes being the ordinary result of inflammation.
Baumgarten, from a very elaborate series of experimental studies, has described the Origin of the various constituents of the tubercle, and their relation to the bacilli, When bacilli' invade a tissue the fixed cells of the tissue, those of epithelium as well as of connective tissue, first show evidences of change. They are induced to proliferate by the bacilli which may be in their substance or in their neighbourhood. The nuclei of these cells show karyokinetic figures, and both giant-cells and epithelioid cells result from the changes in the fixed cells of the tissues. In the case of the giant-cell the nuclear division goes on, but the cell division does not ensue, there being thus a kind of arrest of development. By this process a rounded tubercle arises which is composed entirely of giant-cells and epithelioid cells. But the neighbouring blood-vessels are affected by the virus, and from them an emigration of leucocytes occurs. The leucocytes are at first outside the large-celled tubercle, but penetrate into it, and may convert it into a small-celled or lymphoid tubercle. This transformation may be rapid or slow, its course depending on the number and energy of the bacilli. If the latter are abundant and vigorously propagating, or if they are accompanied by other foreign microbes, then the production of leucocytes may be very great, and the tubercles rapidly pass into the small-celled condition. This may occur so rapidly that the large-celled condition may be almost omitted. Hence it is where the bacilli are comparatively few and the cultivation pure that the large-celled non-inflammatory tubercle is most typically seen.

Fig. 128. - Tubercle showing constituents. A giant-cell is in the middle, and a smaller one lower down. Epithelioid cells form the rest of the tubercle except at the margins, where leucocytes are present.

Fig. 129. - Photograph of a tubercle from the synovial membrane with two giant-cells, x 120.
Bodies having a structure similar to that of tubercles may be produced by the presence of small foreign bodies (rabbit hairs, Baumgarten; particles of stone, Hamilton), but in all such cases the lesions have not an infective character. A more near approach to the true tubercle is met with in Actinomycosis, where the presence of a microbe has the effect of producing results not unlike those of tuberculosis (see Actinomycosis).
The typical tubercle, as here described, is not infrequently difficult of recognition in actual cases. Inflammatory processes occurring around and invading it, obscure its structure, and the tubercle itself is prone to degenerative changes.
Caseous necrosis or Caseation is the most characteristic change in tuberculosis. As already described, this change consists in necrosis with fatty degeneration of the structures. It manifests itself in a granular condition of the cells, whose nuclei disappear. The result is an obscuration of the structure, and the replacement of it by a homogeneous structureless and somewhat opaque material. This change usually begins in the central parts of the tubercles and produces an opacity there, but it is liable to overtake the whole structure. Indeed, it extends to the parts around, so that the tissue which is merely infiltrated with inflammatory products is frequently involved in the caseation. Hence, when the process has overtaken a considerable portion of tissue, the structure may be much obscured. This process in the rapidity and completeness of its occurrence depends on the abundance and vigour of the bacilli. Where they are numerous, and where consequently there is much infiltration with leucocytes, caseation is rapid (Baumgarten). The caseous material so produced is a yellow, brittle substance, which resembles cheese in its appearance. So characteristic is this result of tuberculosis that caseation is almost equivalent to the older term Tuberculization, and caseous matter to Crude or Yellow tubercle.
In very acute cases we may have an approach to ordinary necrosis or sloughing, or at least an acute softening.
The process of caseation is to be related to the action of the virus. It is a necrosis due to the toxic action. Some have endeavoured to account for the caseation by the absence of vessels in the tubercles. But much larger pieces of matter may be kept alive in the body without the intervention of vessels, such as free bodies in the joints or abdomen. Besides, the caseation extends beyond the tubercles to the tissue around, which is vascular.
Fibrous transformation is a much more unusual change in tubercles, and occurs only where the process is very chronic and the bacilli very few. While some tubercles undergo caseation, others, and along with them the surrounding tissue, develop fibrous tissue, like that in chronic inflammation.
Softening is the usual result of caseation. The caseous matter, although it may remain for a time unaltered, in most cases ultimately liquefies or breaks down. The result is the formation of a Cavity or Ulcer. (See Fig. 130.) It is to be remembered that, as the caseation involves not only the tubercles but the surrounding tissue, the cavity or ulcer is associated with an absolute loss of tissue. The walls of the ulcer are tubercular, and the disease usually continues advancing, so that the ulcer or cavity enlarges.
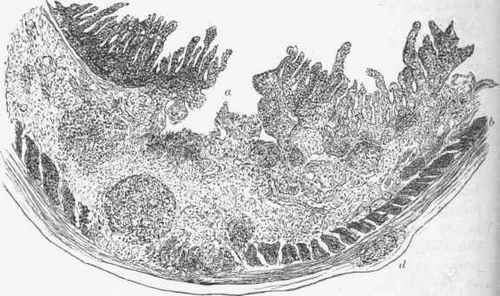
Fig. 130. - Tubercular ulcer of intestine. The rounded form of the tubercles around the ulcer (a) is seen, some of them breaking up the muscular coat (6); one (rf) outside this coat, and beneath the peritoneum, x 16.
On the other hand, the caseous matter may accumulate without softening, and we may have considerable masses of it, such as we find in the brain in the form of the tubercular tumour or scrofulous tubercle and in the lymphatic glands. In course of time the caseous matter may be partly absorbed, or may undergo Calcareous infiltration.
Continue to:
My Books

