Physical Examination of Rectum
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Physical Examination of Rectum
Presumably the patient will have come to the office prepared or the enema will already have been given in the office, and thus the patient will be ready for examination at this point.
If this is not the case, the enema should be given and an interval of about ten minutes allowed for complete evacuation.
1. Inspect the perianal area and do the digital rectal examination (Fig. 25). If this is being done as part of a complete physical survey in the male, it will already have been accomplished at the time of the prostate examination (see p. 61).
2. Prepare the patient for sigmoidoscopy
(a) Explain to the patient what you are going to do and what sensations he or she may experience. Encourage him or her to relax as much as possible to reduce discomfort and to speed the examination. Emphasize especially the necessity of not changing position during examination. Inform the patient that he or she will feel a fullness in the rectum, as well as perhaps some discomfort, and may experience a sensation of gas or cramping in the lower anterior abdomen but that he will not have a bowel movement.

Fig. 25. Inspection of the perianal area and digital examination of the rectum.

Fig. 26. Knee-chest position assumed by the patient for sigmoidoscopy. Weight should be borne on the left shoulder with the head turned to the right and the right arm relaxed.

Fig. 27. Lateral Sims' position may also be used for sigmoidoscopy in selected cases.
(b) Place the patient in the knee-chest position on the examining table as shown in Fig. 26. When the knee-chest position is contraindicated by orthopedic or cardiorespiratory conditions, a lateral Sims' position may be used (Fig. 27).
(c) Arrange drapes over the buttocks.
(d) Repeat the digital examination. This provides an opportunity to check the findings in another position. It also prepares and lubricates the anal canal and helps to relax the sphincter.
3. Check your equipment. Make certain that the light and suction apparatus works before the sigmoidoscope is inserted in the rectum.
4. Do the sigmoidoscopy.
(a) Lubricate the instrument.

After digital palpa-tion of the anal canal. Introduce the well-lubricated sigmoidoscopo with firm gen-. tle pressure until tho tip is a few centimeters within the rec tum.
Remove the obtura-tor, adjust the light, and advance the sigmoidoscope under direct vision. At "blind pockets" withdraw the Instrument a few cantimeters until the lumen reappears, and then proceed. Remove the retained fluid or mucus by suction when necessary.
Use tho insufflator sparingly. If at all. The primary use of air is to flatten folds to assure fall visualisation during withdrawal of the sigmoidoscope.
Fig. 28. Technique for sigmoidoscopy. A, Insertion of the sigmoidoscope. B, Use of suction. C, Insufflation of the bowel with air.
(b) Insert the sigmoidoscope a few centimeters inside the rectum with the obturator held firmly in place (Fig. 28, A).
(c) Remove the obturator and adjust the light.
(d) Observe the contour and axis of the rectum where die sigmoidoscope is situated. The normal axis is up and toward the left.
(e) Suction may be required to remove secretions or retained enema fluid (Fig. 28, B).
(f) Advance the sigmoidoscope under direct vision, following the contours of the bowel.
(g) If a "blind pocket" is encountered, withdraw the sigmoidoscope a few centimeters until the lumen reappears, and then proceed.
(h) Pass the instrument to its full length with deliberate speed and caution.
(i) Insertion of the scope to its full length should be accomplished in most patients who do not present bowel abnormality. In some patients, particularly those who have had lower abdominal surgery, fixation or angulation of the bowel makes insertion beyond 16 to 18 cm. impossible without undue discomfort. To overcome physiologic spasm and resistance to passage of the sigmoidoscope, the following steps are usually effective:
(1) Maintain steady gentle forward pressure. Force should never be used.
(2) Assure the patient that it is natural to feel a fullness in the rectum "as though the bowels were going to move" and that this should not be alarming or resisted.
(3) Instruct the patient to take a few deep breaths slowly.
(4) Insufflate the bowel with air (Fig. 28, C). Air should be used only when clearly necessary during introduction of the sigmoidoscope, and then only sparingly and gently, not explosively.
(j) Remember that it is better to accomplish a safe and relatively comfortable examination of the rectum and colon, limited to 16 or 18 cm. on the asymptomatic patient, than to cause the patient so much pain that he or she vows never to submit to the procedure again, with or without symptoms. This would defeat the whole purpose of the examination.
(k) At the maximum distance of insertion, note particularly the presence of any blood or blood-tinged mucus coming from beyond the sigmoidoscope.*
(1) Remove the sigmoidoscope in a rotary fashion, visualizing the entire circumference of the bowel in the process (Fig. 29). (m) Air insufflation is helpful in distending the bowel and flattening the mucosal folds for better visualization. It should be used sparingly and only if necessary for thorough inspection.
(n) Particular attention should be given to the relatively blind presacral area of the rectum, as well as to those regions just behind the several mucosal valves.
(o) Remove the sigmoidoscope.
*This finding indicates the need for x-ray studies of the colon above the level of sigmoidoscopy.




Remove the sigmoidoscope in a rotary fashion, visualising the entire circumference of the bowel.
Use air insufflation only if necessary to separate mucosal surfaces.
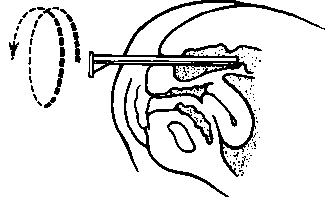
Fig. 29. Removal of the sigmoidoscope in a rotary fashion.

Fig. 30. Technique of anoscopy.
5. Do an anoscopy.
(a) Insert the anoscope (Fig. 30). Turn the instrument gently in rotary fashion and inspect the anal canal. The headlamp is a good source of light for this procedure. Anoscopy may be omitted if digital examination is negative and the area was visualized while withdrawing the sigmoidoscope.
Continue to:
My Books

