Screening Presumably Well Women For Breast Cancer-Detection
Description
This section is from the book "Early Detection And Diagnosis Of Cancer", by Walter E. O'Donnell. Also available from Amazon: Early Detection And Diagnosis Of Cancer.
Screening Presumably Well Women For Breast Cancer-Detection
Inspection and palpation are the only practical methods of surveying women for breast cancer. Periodic x-ray examination of the breast (mammography) has been proposed by some, and it is under intensive investigation at this time. Its value remains to be determined.
As described on pp. 55 to 60 periodic breast examination can be done by either the physician or the patient, preferably both. Where periodic examination is not practiced as a routine, over 90% of all breast cancer is discovered accidentally by the patient. Since it is not feasible to provide for frequent, regular breast examination of all women by physicians, the need for encouraging breast self-examination is obvious. As a result of periodic self-examination, it is possible for women to discover breast masses months earlier than if they rely on chance alone.
Clinical Features Of Breast Cancer-Diagnosis. Localized Lesion. Symptoms
1. Usually none. The lesion may be noted during routine examination.
2. The fortuitous finding of a lump or mass by the patient most commonly brings her to the doctor's office. The lesion itself usually produces no symptoms.
3. Occasionally the patient's attention may be drawn to the breast by the occurrence of mild discomfort, pain, or fullness.
Signs
1. A lump or mass in the breast is almost invariably the first sign. This may be visible as well as palpable. If it is known to be of recent origin, it takes on added significance. This may take the form of:
(a) A discrete nodule in an otherwise normal breast
(b) A dominant mass within a breast displaying diffuse or multiple nodules
(c) A hard mass in a normal or abnormal breast
2. Occasionally a spontaneous nipple discharge, especially one which is bloody, may be noted. This is relatively uncommon and, when present, most often signifies an intraductal papilloma. However, it may signify an underlying papillary carcinoma.
3. Unilateral scaling, crusting, or excoriation of the nipple should suggest the diagnosis of Paget's disease which in turn reflects an underlying ductal carcinoma.
4. Retraction phenomena. These are, of course, far more obvious in advanced breast cancer but, if looked for carefully, can be demonstrated in many localized lesions as well.
These retraction phenomena reflect the tendency of breast cancer to be surrounded by fibroblastic proliferation. This fibrotic reaction exerts tension on the fascia and connective tissue stroma of the breast and produces dimpling, depression, or irregularity of the overlying skin (and occasionally deviation or inversion of the nipple). These signs may be unimpressive and almost undetectable. The most important thing about them may be their asymmetry; i.e., they are present in one breast and absent in the other.
Retraction signs may become apparent during the course of the routine breast examination as described on p. 55, especially when the patient is seated and the arms are raised above the head. Often, however, in the case of a relatively small, localized breast lesion, they may be demonstrable only as a result of certain provocative maneuvers. These include the following:
(a) With the patient seated and with her hands on her hips, have her tense the pectoral fascia (by pressing her hands against her hips) (Fig. 48, A). The normal breast may be expected to rise slightly; the affected breast (or just the abnormal part of it) will be pulled upward sharply. Deviation of the nipple toward the lesion and accentuation of the skin dimpling or depression may be noted also.
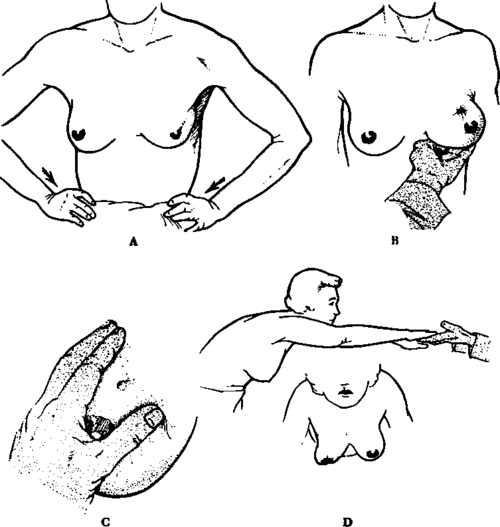
Fig. 48. Techniques used in demonstrating retraction phenomena in localized lesions of the breast.
(b) With the patient in an upright position, the examiner lifts the breast from below with the palm of his hand (Fig. 48, B). The surrounding breast will relax while the skin adjacent to the lesion may display dimpling or depression.
(c) With the patient in either an upright or recumbent position, the examiner gentiy grasps the lesion between his thumb and index finger and relaxes the skin across it (Fig. 48, C).
(d) Have the patient stand up and lean forward with her head upright, her hands extended forward as far as possible, and her fingers resting on the outstretched hands of the examiner. With the patient in this position the breasts fall free of the chest, and the physician observes them for any asymmetry or retraction phenomena.
Advanced Lesion
The clinical manifestations of advanced breast cancer can be divided into three categories: progression of local signs, evidence of regional metastasis, and evidence of distant metastases.
Progression Of Local Signs Or Symptoms
1. Large, bulky tumor
2. Skin edema (orange peel or pigskin appearance)
3. Venous pattern over the breast surface
4. Obvious retraction phenomena; fixation to skin and/or chest wall
5. Ulceration; secondary infection
6. Pain
7. Satellite skin nodules
8. Local inflammatory response
Evidence of regional metastases
1. Enlarged axillary nodes
2. Enlarged supraclavicular nodes
3. Edema of the upper extremity
4. Involvement of the opposite breast
5. Horner's syndrome (see p. 127)
Evidence of distant metastases
1. Lesions in bones
(a) Usually osteolytic but may be osteoblastic or a mixture of both
(b) Most common in the spine, pelvis, and ribs but may occur anywhere
(c) Symptoms of pain, etc., may precede by weeks or months x-ray demonstration of lesions
(d) Pathologic fracture or nerve root involvement may be present
(e) Clinical syndrome of hypercalcemia may occur
2. Lesions in the lungs and/or pleura
(a) Nodular densities in one or both lungs
(b) Pleural effusion
(c) Occasional miliary or diffuse lymphangitic spread in the lung
(d) Cough, dyspnea, or pleural pain may be prominent symptoms
3. Lesions elsewhere
(a) Liver-gross enlargement, nodularity, and later jaundice
(b) Peritoneum-ascites and related gastrointestinal complaints
(c) Brain-associated central nervous system symptoms and signs
(d) Heart-associated arrhythmia, pericardial involvement, and decompensation
Continue to:
My Books

