Adrenal Support Of Human Mammary Cancer
Description
This section is from the book "The Scientific Contributions Of The Ben May Laboratory For Cancer Research", by The University of Chicago. Also available from Amazon: The Scientific Contributions Of The Ben May Laboratory For Cancer Research.
Adrenal Support Of Human Mammary Cancer
Cancer of the breast is one of the most noble of the problems of cancer; in the United States it has the highest rate of incidence of any cancer of either sex.
In 1896, Beatson (Lancet, 2:104, 1896), on empirical grounds, postulated that ovarian "irritation" was a factor in mammary cancer and performed ovariectomy on two women suffering from cancer of the breast; some regression of the tumors was observed in these cases.
The concept that hormones of the adrenal gland can sustain human mammary cancer was based on four considerations: (a) In certain stocks of mice from which the gonads had been removed at an early age, adrenal hyperplasia and tumors develop, and cancer of the breast arises subsequently (Woolley, G. W.; Fekete, E.; and Litde, C. C. Proc. Nat. Acad. Sc., 25:277, 1939). (b) Certain patients with adrenal tumors excrete large amounts of steroids similar to those elaborated in the ovary, (c) Following orchiectomy in cancer of the prostate, the excretion of 17-ketosteroids in the urine often is increased, (d) The adrenals are the gonads of the aged.
Total adrenalectomy in patients with malignant disease was first performed in 1945 (Huggins, C, and Scott, W. W. Ann. Surg., 122:1031, 1945), but the postoperative management was difficult and hazardous to the patient. When cortisone became available in adequate supply, the problem was reinvestigated. A surgical technique was devised for total adrenalectomy in man (47) in a single stage, and a hormonal substitution program (42) was elaborated for his maintenance thereafter." Cortisone made possible this satisfactory replacement regimen. When maintained adequately, adrenalectomized patients have a healthy appearance, are not incapacitated, and they are able to engage in all of their usual activities. Cutaneous pigmentation of the Addisonian type does not occur. Often adrenalectomy incites the onset of vasomotor hot flushes. In a proportion of cases cancers regress profoundly. A second indication for total adrenalectomy is Cushing's disease (47).

Fig.1.-The first patient in whom regression of widespread cancer of the prostate followed hormonal control (Mr. A.J. preoperative).

Fig. 2.-X-rays of Mr. A.J. 8 years after orchiectomy; note healing of the metastases.

Fig. 3.

Fig. 4.
Fig. 3.-Metastases of cancer of prostate in inguinal lymph nodes Fig. 4.-The same patient 8 years after orchiectomy.
In prostatic cancer, perhaps the most striking observation was the immediate and persistent relief of crippling pains in the bones after adrenalectomy. Regression of the tumor of considerable magnitude was seen in a small number or patients. In mammary cancer, regression after adrenalectomy is more common than in patients with prostatic cancer.
In our first series, adrenalectomy was performed in 52 patients with metastatic mammary cancer; there were two postoperative deaths. The basis for selection of these patients was (a) extensive and proven mammary cancer with (b) failure to respond to earlier methods of treatment. No other discriminatory tests were applied, and no patient was refused operation because of the severity of the disease.
' Collaboration with the late D. M. Bergenstal was close and fruitful in this venture. We mourn the premature loss of this fine man and clever endocrinologist (J. Nat. Cancer Inst., 33 [November] III, 1950).

Fig. 5.-In metastatic cancer of the prostate, stilbestrol induced a decline of serum acid phosphatase.
(--), and a concurrent rise of alkaline phosphatase, (----), as regression of the neoplasm took place.
(Cancer Research, 1:293, 1941).
Assessment of remission was based on both subjective and objective evidence of improvement. Objective remission was measured by regression (Figs. 6 and 7) or disappearance of obvious and easily accessible lesions, such as cutaneous metastases and intra-abdominal masses, and also by X-ray evidence of calcification of osteolytic lesions, the healing of fractures or disappearance of pulmonary lesions and pleural fluid. Objective remission occurred in 40 per cent (20 of a total of 50 patients). Subjective improvement was often equally remarkable, especially in the relief of bone pain, disappearance of respiratory difficulties, and return of a sense of well-being. The remissions were of varying duration from 6 months to more than 8 years. Obviously certain patients with mammary cancer respond in a gratifying manner to adrenalectomy, while others have cancers which are not hormone-dependent.
A study was made of criteria of beneficial response of clinical mammary cancer to adrenalectomy, and this has proved to be helpful in the selection of responsive patients for adrenalectomy. (1) The greatest relief was observed in men or women 40-70 years of age. (2) A prolonged interval between mastectomy and manifestations of recurrence of the cancer; the rapidity of growth of a cancer indicates its degree of malignancy. The hormone-dependent mammary cancers commonly are not explosive in their growth rate. (3) An appreciable titer of estrogenic substances in the urine is an important criterion of possible future benefit from adrenalectomy. (4) The hormone-dependent mammary cancers are commonly well-differentiated cytologically, being composed largely or entirely of glands, surrounded by myo-epithelial cells, and they contain milky secretion in their lumina.
In brief, adrenalectomy with maintenance of the patient on cortisone has caused an appreciable regression of far-advanced mammary cancers for which no other therapy was available. In a small number of patients in the terminal stage of the disease, remissions have lasted for more than eight years. It is established that hormones produced by the adrenal glands are components which sustain and propagate certain mammary cancers of the human male and female.
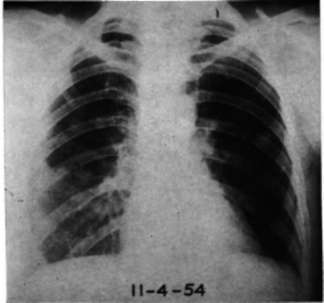
Fig. 6.-Metastases of cancer of the breast to lung and pleura.

Fig. 7.-Same patient 5 years after adrenalectomy.
Continue to:
My Books

